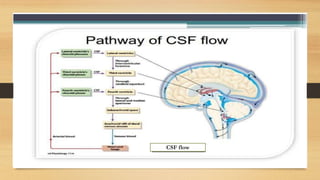
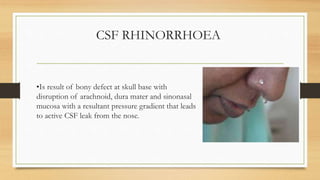
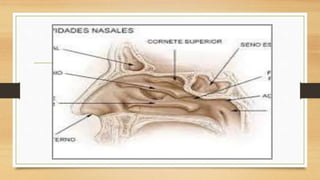
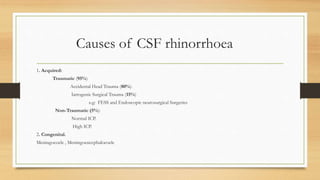
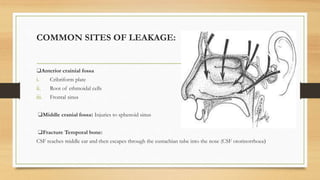
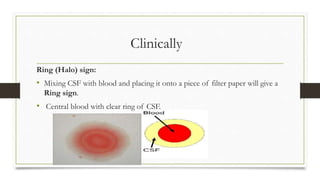
This document discusses cerebrospinal fluid (CSF) rhinorrhea, which occurs when there is a defect in the skull base that allows CSF to leak into the nose. The main causes are traumatic head injury or surgery near the skull base. Symptoms include clear nasal discharge that increases with straining. Diagnosis involves imaging, laboratory tests, and examination maneuvers to detect increased CSF pressure. Conservative management aims to decrease CSF pressure through bed rest, medications, and lumbar drainage. Surgery is needed if conservative measures fail or for large defects. Surgical repair involves using an endoscopic or open approach to graft the defect and stop the CSF leak.