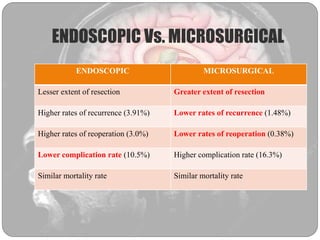
Colloid cysts are benign tumors located in the anterior third ventricle that can cause hydrocephalus. They arise from ependymal or choroid plexus cells. Common symptoms include headache, nausea, and gait disturbances. On imaging, colloid cysts appear hyperdense on CT and hyperintense on T1-weighted MRI. Treatment options include conservative management, shunting, and surgical resection via transcallosal or transcortical approaches. Endoscopic resection has lower risks but higher recurrence rates compared to microsurgery. Complications of surgery include venous infarction, mutism, and CSF leaks.