Downloaded 40 times

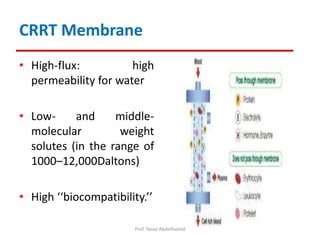
![Why
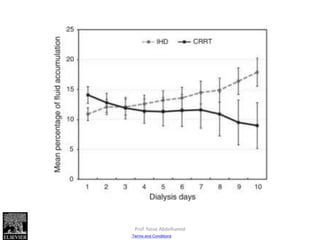
• Maintenance of intravascular compartment volume
• Prolonged treatments permit lower fluid removal rates
– IHD: 3 L in 3 hours = 1 L/h UF rate
– CRRT: 3 L in 24 hrs = 0.125 ml/h UF rate
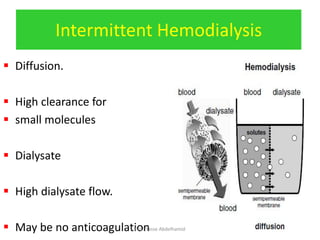
• Urea diffusion is faster with IHD than CRRT
– IHD: Urea clearance ~160 ml/min
– CRRT: Urea clearance ~15-30 ml/min
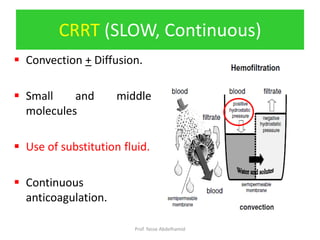
• Convective sodium removal rate
[hemofiltration/hemodiafiltration] is less than diffusive
removal rate [hemodialysis]
• Decreased core temperature.
• Convective removal of inflammatory mediators could
contribute to hemodynamic stability.
Prof. Yasse Abdelhamid](https://image.slidesharecdn.com/crrtindicationsandmodalitiesautosaved-181208052139/85/Crrt-indications-and-modalities-autosaved-8-320.jpg)

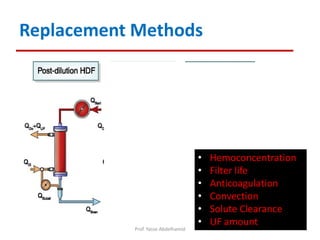

![Relative indications:
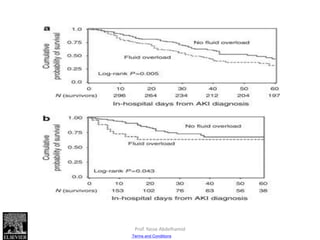
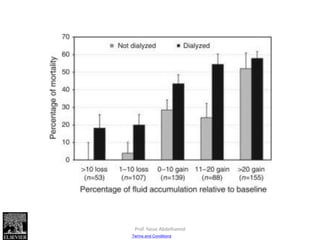
–Fluid overload (diuretic sensitive)
–BUN >76 mg/dl (27 mmol/l)
–[Serum Na+] < 110 and >160 mmol/L
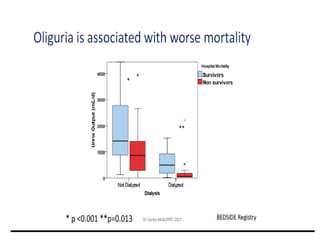
–Oligurea: RIFLE class R, I, F.
INDICATIONS
Prof. Yasse Abdelhamid](https://image.slidesharecdn.com/crrtindicationsandmodalitiesautosaved-181208052139/85/Crrt-indications-and-modalities-autosaved-32-320.jpg)

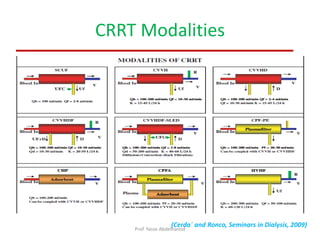
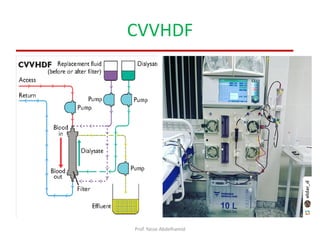
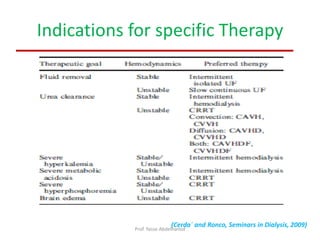
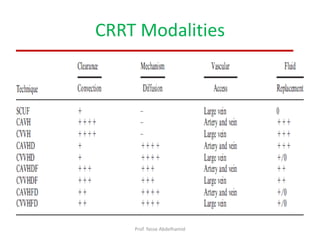
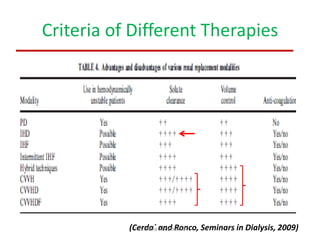

The document discusses continuous renal replacement therapy (CRRT) modalities for acute kidney injury (AKI) patients in the intensive care unit (ICU). It provides details on different CRRT modalities including CVVH, CVVHD, and CVVHDF. CVVHDF is described as the safest combination as it utilizes both diffusion and convection. The document also discusses indications for specific CRRT therapies and notes that patient hemodynamic stability is the main determinant for choice of dialysis modality.











































![Continuous rrt and its role in critically ill patients [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/continuousrrtanditsroleincriticallyillpatientsautosaved-180707065857-thumbnail.jpg?width=640&height=640&fit=bounds)











































