What is RenalReplacement Therapy
(RRT)?
• Replaces kidney function to remove waste,
balance fluids and electrolytes
• Used in ICU patients with acute kidney injury
(AKI)
4.
Understanding Kidneys andNephron
• Kidneys filter ~180 liters of blood daily
• Each kidney contains ~1 million nephrons
• Nephrons include a glomerulus and renal
tubules
• Functions: waste removal, fluid &
electrolyte balance, acid-base regulation
Acute renal failure,also known as
acute kidney injury (AKI)
abrupt (within 48 hours) reduction in kidney
function. The AKI network defines the
reduction in kidney function as the presence
of any one of the following:
• An absolute increase in serum creatinine of
≥ 0.3 mg.dl-1 (≥ 26.4 mcmol.l-1)
• A percentage increase in serum creatinine
of ≥ 50% (1.5-fold from baseline)
• A reduction in urine output (< 0.5 ml.kg-1 per
hour for more than six hours).
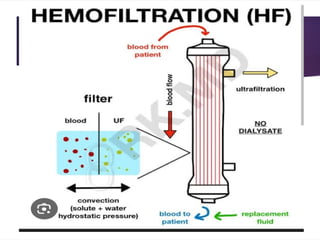
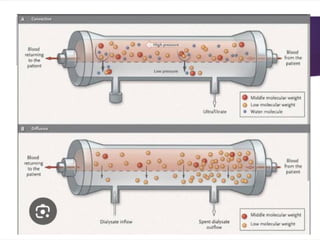
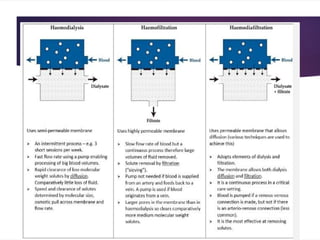
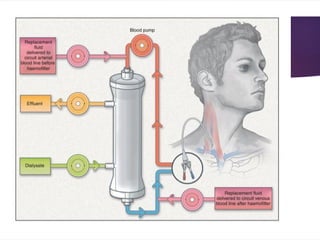
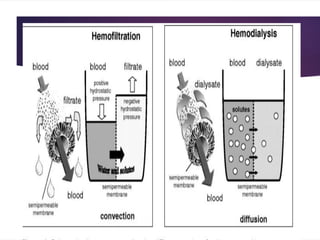
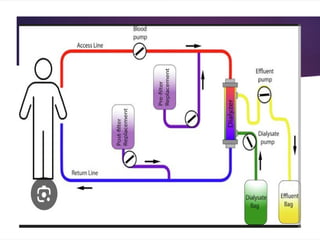
HemoFiltration ( convection)
Haemofiltration= blood being pumped through an extracorporeal
system
semi-permeable membrane
hydrostatic pressure created on the blood-side of the filter
drives plasma water across the filter
This process is referred to as ultrafiltration
Molecules that are small enough to pass through the membrane
(<50,000 Daltons) are dragged across the membrane with
the water by the process of convection.
The filtered fluid (ultrafiltrate) is discarded
replacement fluid is added in an adjustable fashion according to the
desired fluid balance.
14.
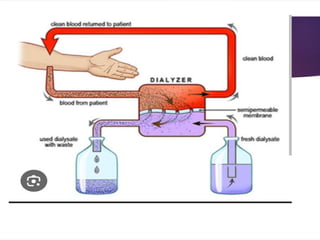
Haemodialysis (diffusion)
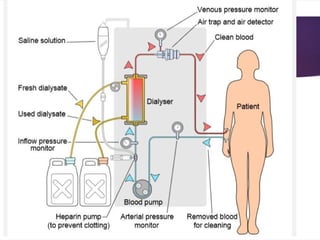
Haemodialysisinvolves blood being pumped through an extracorporeal
system that incorporates a dialyzer.
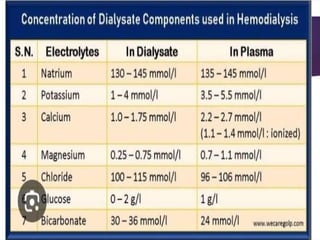
In the dialyzer, blood is separated from a crystalloid solution (dialysate) by
a semi-permeable membrane.
Solutes move across the membrane along their concentration gradient
from one compartment to the other obeying Fick`s laws of diffusion.
For example, bicarbonate moves from dialysate to blood whereas urea and
potassium move from blood to dialysate.
dialysate flows countercurrent to the flow of blood.
When removal of water is required the pressure on the blood-side of the
membrane has to be increased forcing water molecules to pass into the
dialysate.
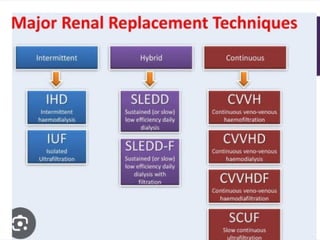
SCUF
Slow continuousultrafiltration is used when the only
requirement is water removal.
Effectively, it is CVVH with a low filtration rate.
It can remove up to 6 litres of fluid a day but solute
removal is minimal.
24.
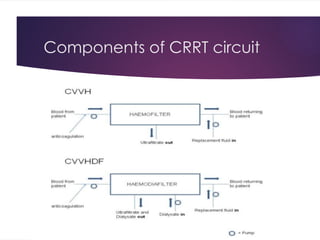
Replacement fluid
Itis a substitution fluid:
A solution of variable composition
physiologic
used to replace large volumes of ultrafiltrate during hemofiltration or
hemodiafiltration.
Replacement fluid may be given as predilution or postdilution."
25.
Dilaysate
A solutionof variable composition designed to facilitate diffusion of solutes into
the ultrafiltrate-dialysate compartment of the hemofilter or hemodialyzer.“
Dialysate is the fluid which is infused into the filter
by convention everything that comes out of the filter is called effluent
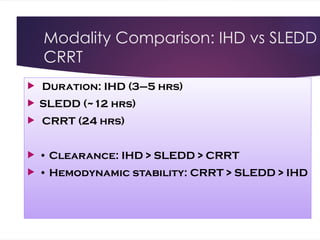
Intetmittent vs Continuous
Dialysing with higher flow rates than CRRT.
A typical regime is 3-5 hours of dialysis 3 times
a week.
The high flow rates and rapid fall in plasma
osmolality mean that it is only suitable for
patients who are cardiovascularly stable.
30.
Continuous mode ofhemodialysis
CRRT involves filtering and/or dialysing on a
continuous basis.
It allows better fluid managemen.
creates less haemodynamic disturbance
more expensive than IHD and requires continuous
rather than intermittent coagulation.
There is some evidence to suggest that CRRT is
superior to IHD in
patients with sepsis, cardiovascular instability or with
a head injury.
31.
SLED
Sustained lowefficiency dialysis is an
example of a hybrid therapy which aims to
combine the logistic and cost advantages of
IHD with the relative cardiovascular stability
of CRRT.
Treatments are intermittent but usually daily
and with longer session durations than
conventional IHD
Solute and fluid removal are slower than
IHD, but faster than CRRT
32.
WHICH FORM OFRRT SHOULD WE US
What we want to remove from the plasma
The patient`s cardiovascular status
The availability of resources
The clinician`s experience
Convective modes of RRT may be beneficial if the patient
has septic shock
• CRRT can aid feeding regimes by improving fluid
management
• CRRT may be associated with better cerebral perfusion
in patients with an acute brain injury
or fulminant hepatic failure
Dialyzer Membranes andPerforman
• Synthetic membranes preferred over
cellulose for better biocompatibility
• Factors: flux, permeability, surface area
• Clears solutes based on size and
transport mechanism
39.
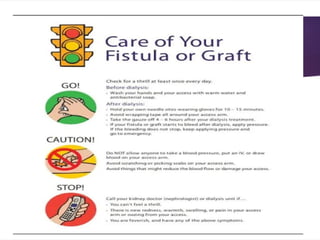
Vascular Access forRRT
• Preferred sites: Right IJV > Femoral >
Left IJV > Subclavian
• Types:
AV fistula
tunneled catheter
temporary catheter
40.
Anticoagulation During RRT
• Systemic: Heparin (risk of HIT, bleeding)
• Regional: Citrate (preferred for
circuit longevity)
• Citrate chelates calcium – monitor for
electrolyte shifts
45.
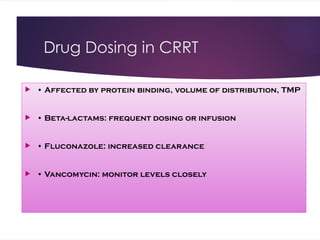
Drug Dosing inCRRT
• Affected by protein binding, volume of distribution, TMP
• Beta-lactams: frequent dosing or infusion
• Fluconazole: increased clearance
• Vancomycin: monitor levels closely
47.
When to StopRRT
• Urine output > 400 mL/day suggests
renal recovery
• Creatinine clearance > 20 mL/min
often used as threshold
• Monitor creatinine trend during
steady-state
48.
Chronic Kidney RiskPost-AKI
• 40% of ICU AKI survivors develop CKD
• Some remain dialysis dependent
• Follow-up nephrology care is essential
49.
Research & Controversiesin RRT
• Timing of RRT initiation: early vs
delayed
• High-volume haemofiltration in
sepsis: unclear benefit
• Need for validated AKI biomarkers
50.
Summary: Key Pointsin RRT
• CRRT preferred in unstable patients
• Know AEIOU indications
• Tailor modality, dosing, and
anticoagulation to the patient
• Watch for complications and long-term
kidney outcomes

























![Continuous rrt and its role in critically ill patients [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/continuousrrtanditsroleincriticallyillpatientsautosaved-180707065857-thumbnail.jpg?width=640&height=640&fit=bounds)

































