Downloaded 148 times


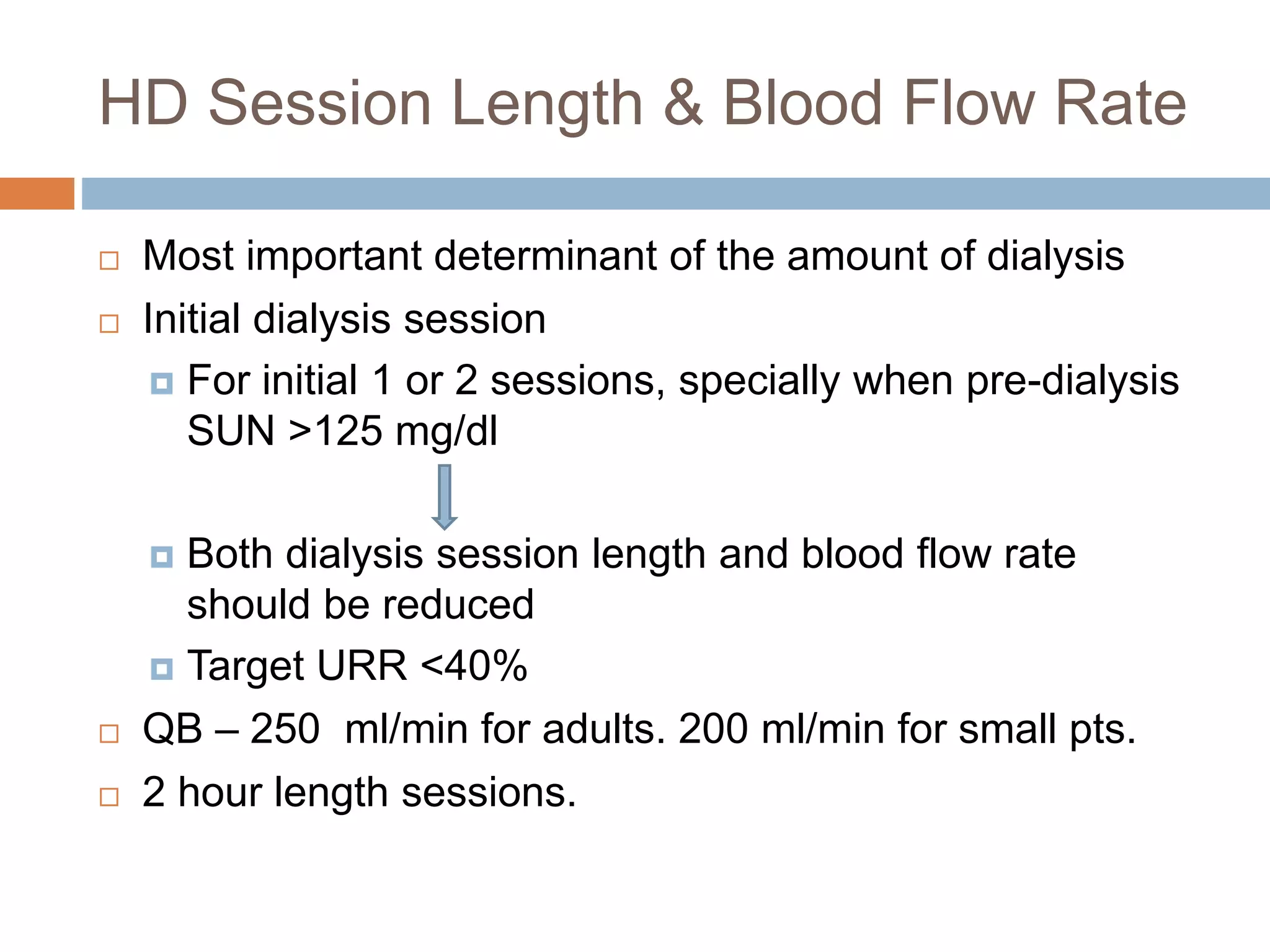


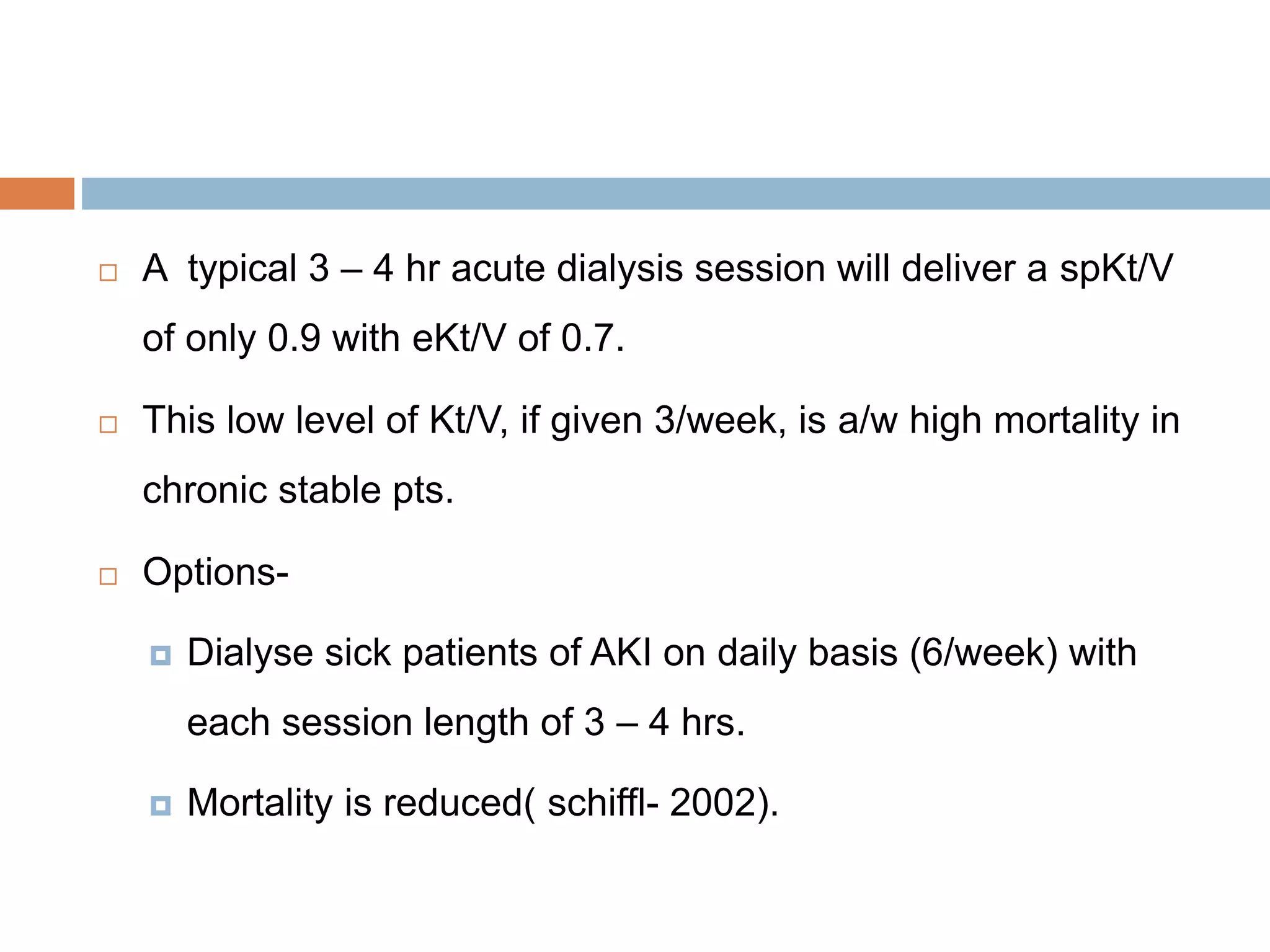





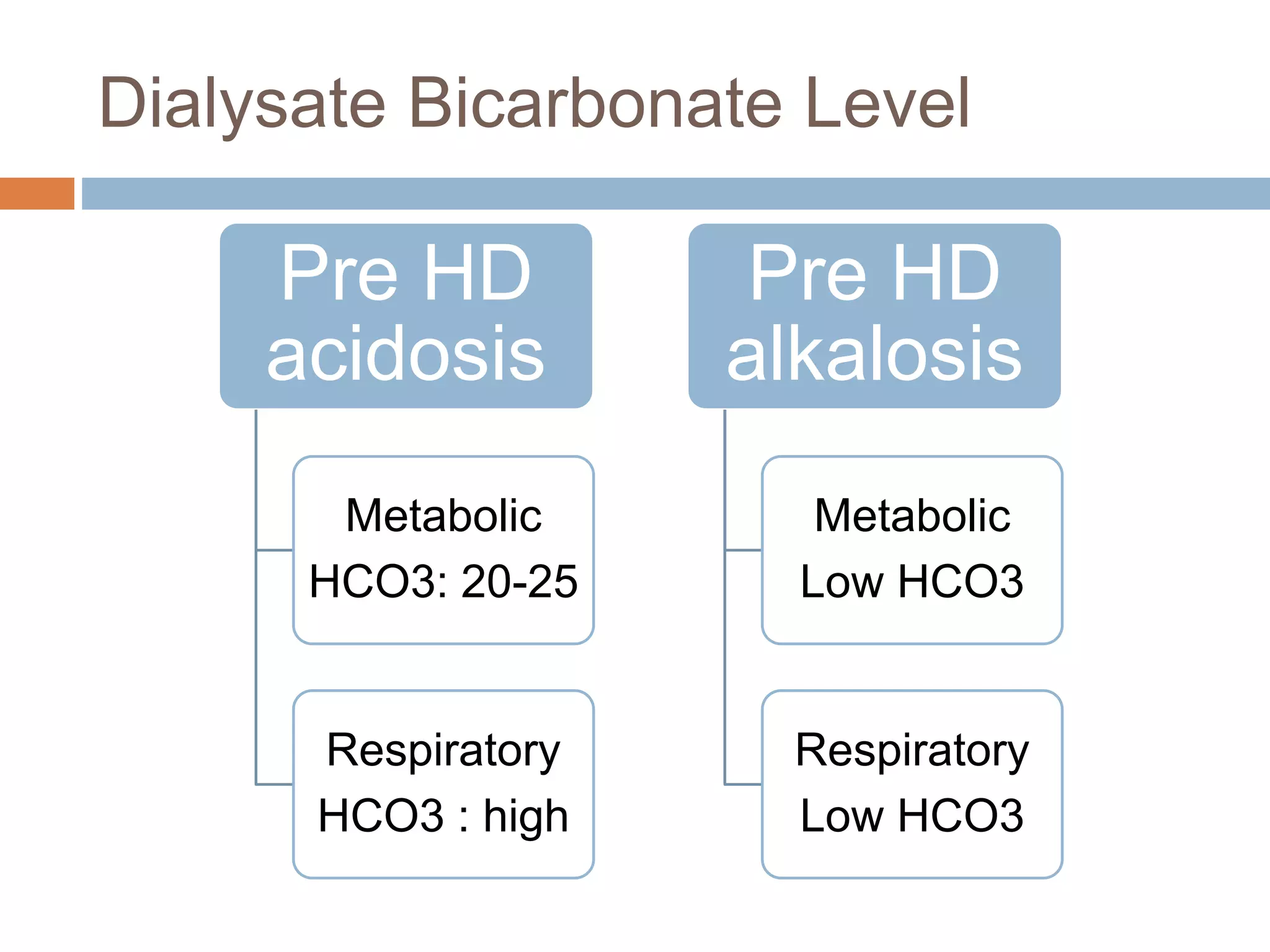









































































This document discusses guidelines for prescribing hemodialysis for acute kidney injury patients. It covers key elements of the prescription including session length and blood flow rate, dialyzer selection, dialysate composition, and ultrafiltration orders. The presentation emphasizes starting more frequent but shorter sessions at lower intensity initially and gradually increasing session length and clearance as the patient stabilizes to prevent dialysis disequilibrium syndrome.























































































