Downloaded 494 times

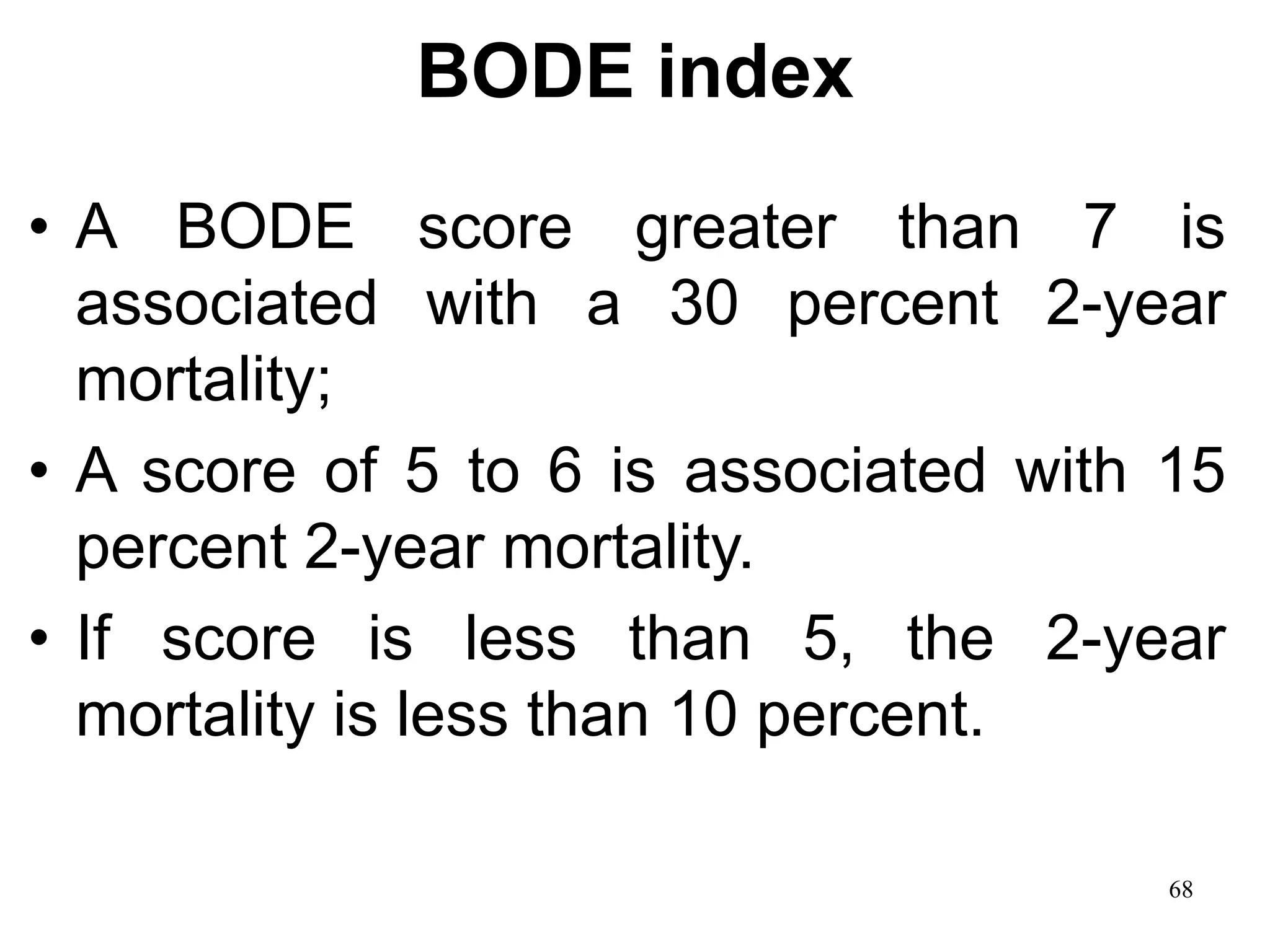
![BODE index
• A multidimensional prognostic index
• Takes into account several indicators of COPD
prognosis (body mass index [BMI], obstructive
ventilatory defect severity, dyspnea severity,
and exercise capacity).
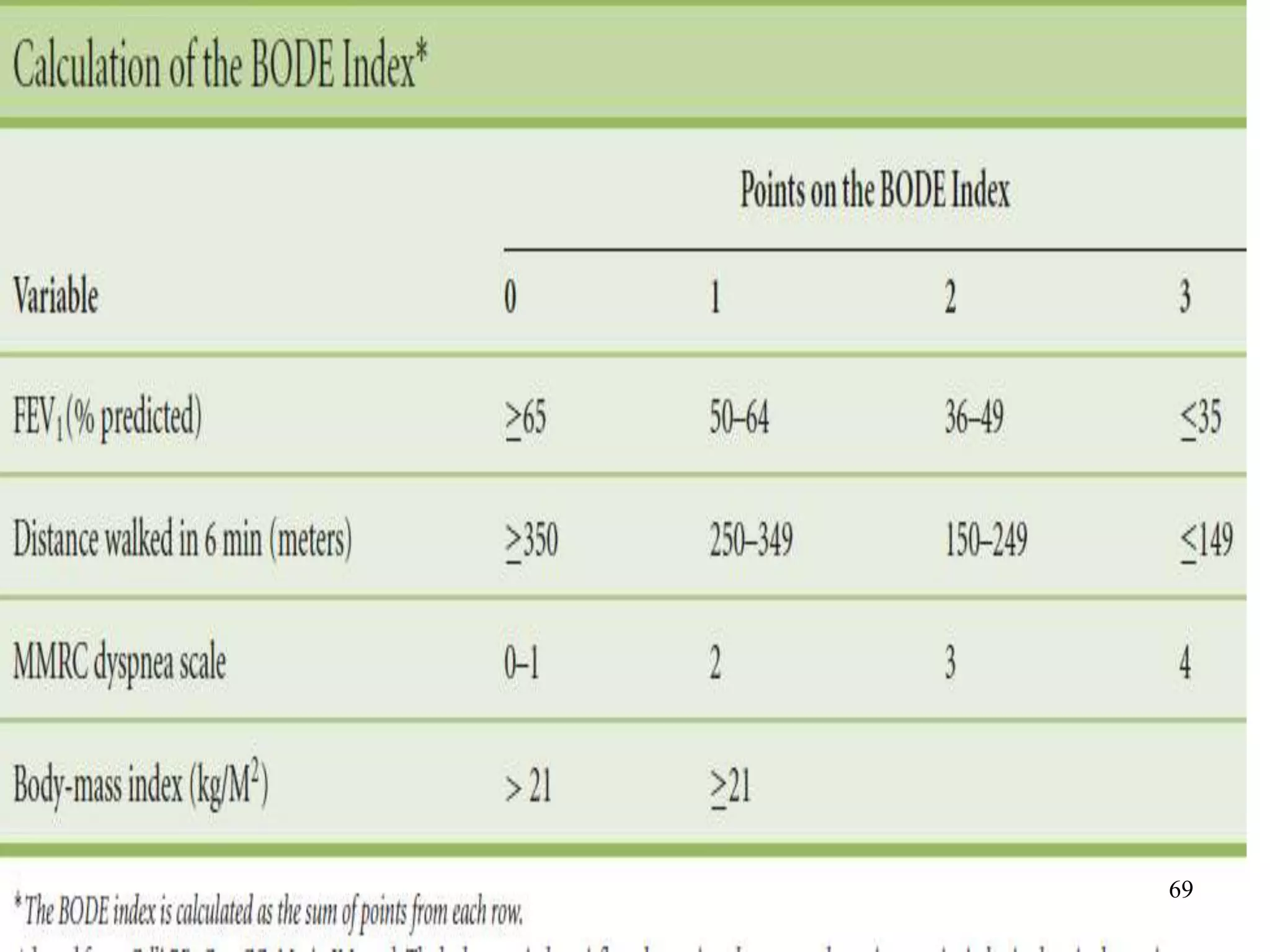
• The components are derived from measures of
the body mass index (weight in kg/heightm2),
FEV1 percent predicted, the modified Medical
Research Council dyspnea and 6 min. walk
Test. 67](https://image.slidesharecdn.com/copdncomorbidities-3-140330103943-phpapp01/75/Copd-n-comorbidities-67-2048.jpg)
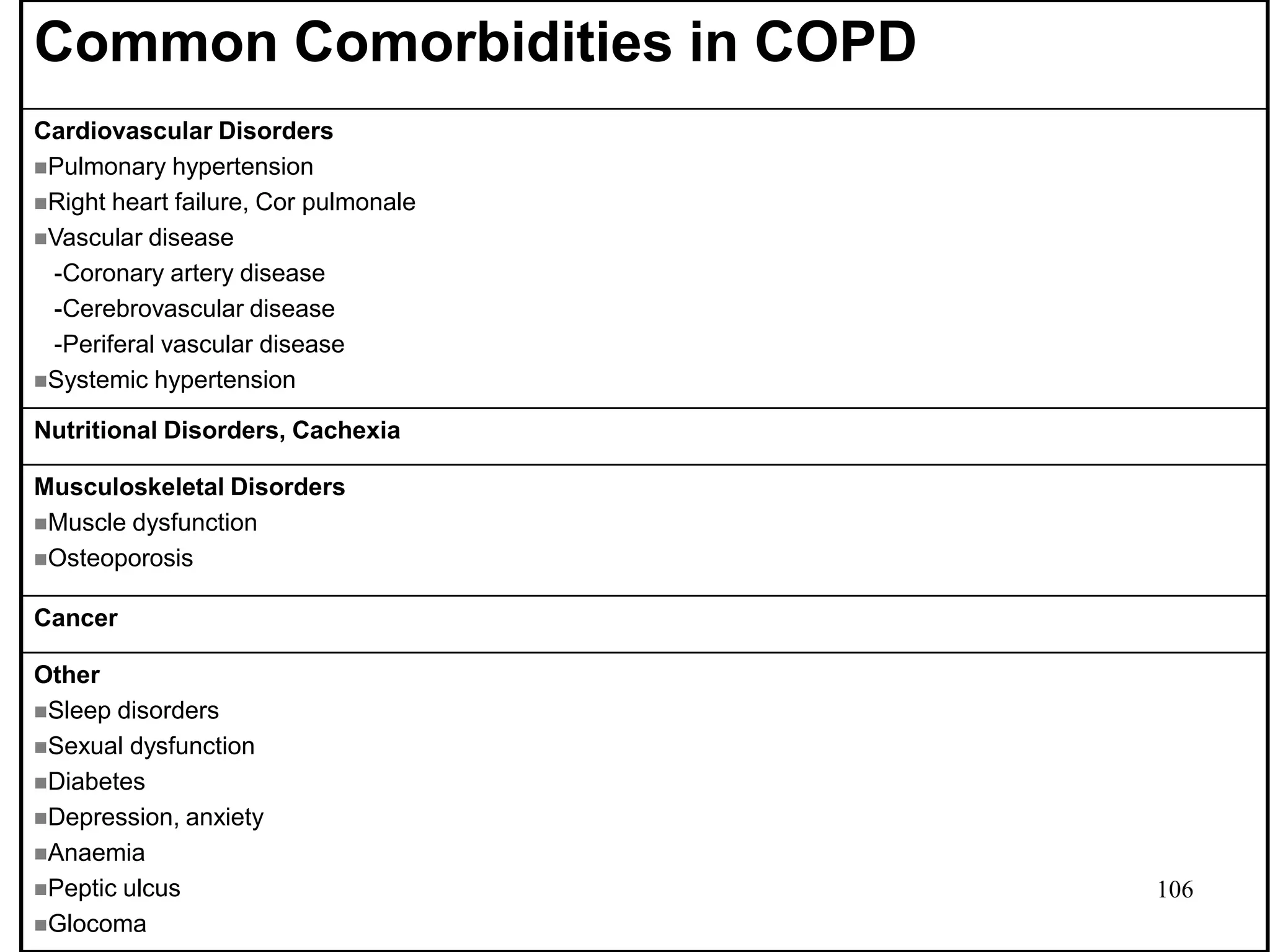


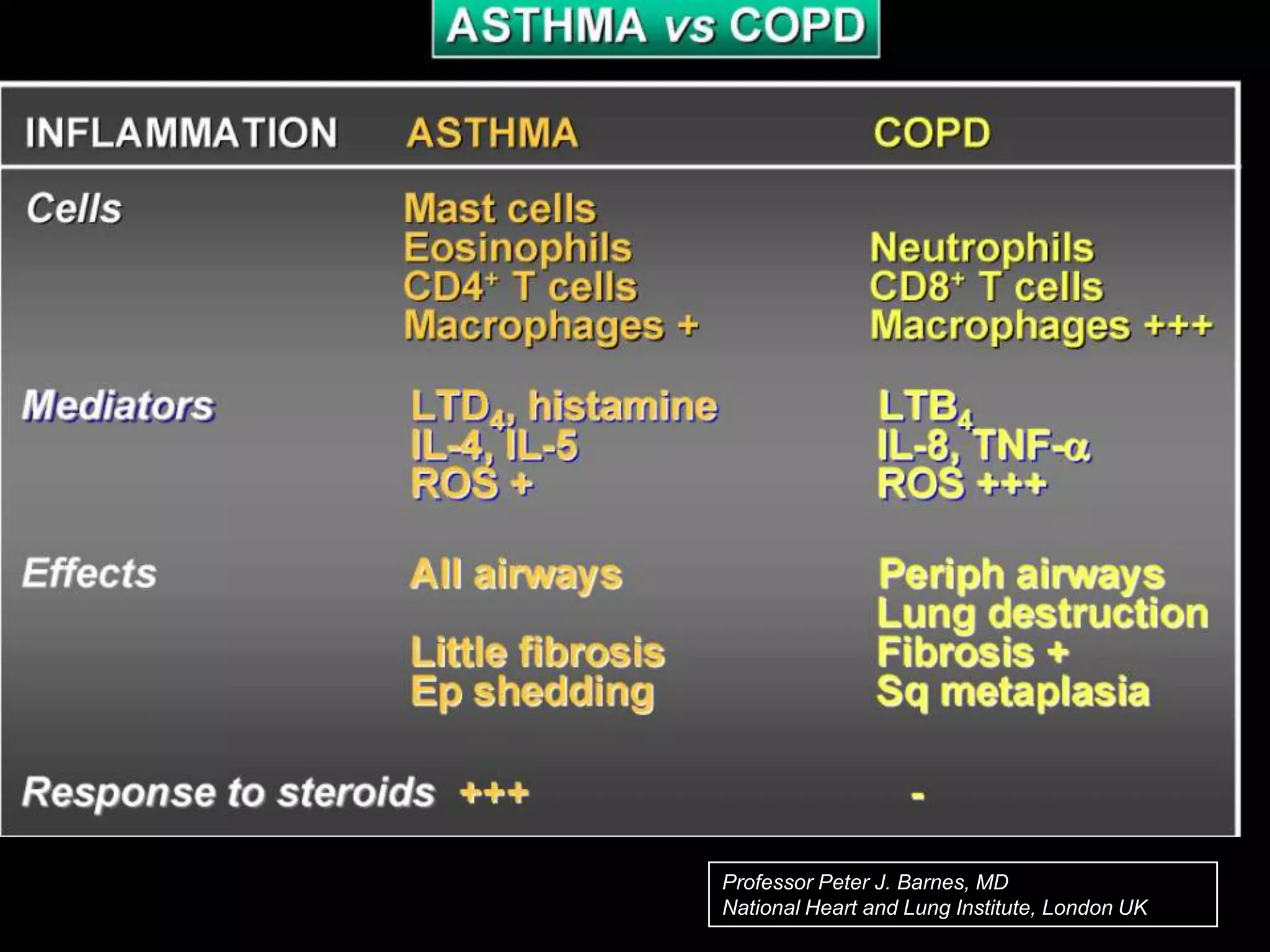
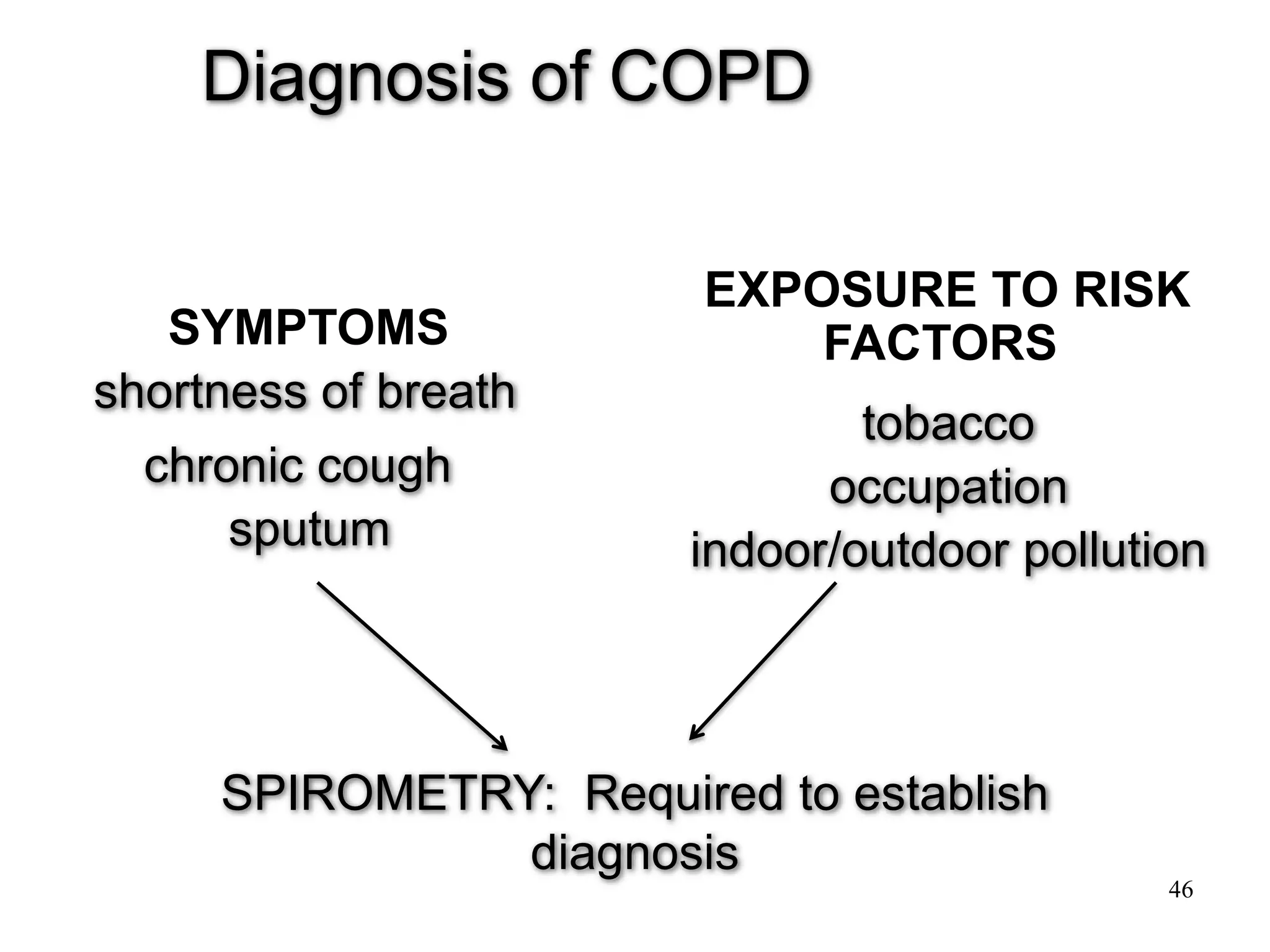
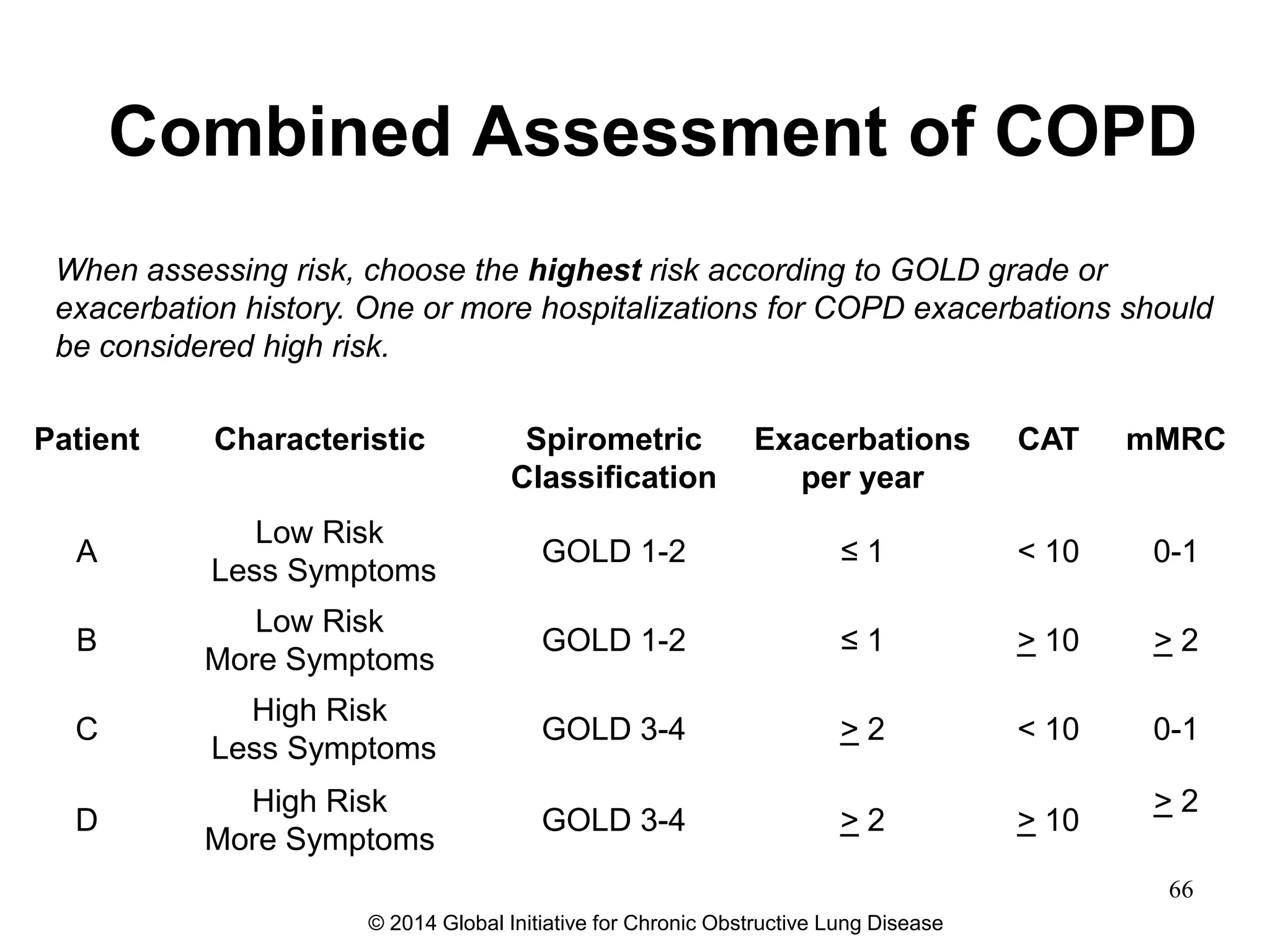
The document discusses COPD and its comorbidities. It defines COPD as a disease characterized by persistent airflow limitation associated with an inflammatory response in the lungs to noxious particles. COPD has several risk factors and a variable natural history. The key pathological changes occur in the central and peripheral airways, lung parenchyma, and pulmonary vasculature. This leads to several physiological abnormalities including airflow limitation, gas exchange impairment, pulmonary hypertension, and systemic effects. Diagnosis requires symptoms, risk factor exposure, and confirmation of persistent airflow limitation on spirometry. Assessment aims to determine disease severity and impact on health status and risk of future events. Comorbidities commonly occur and should be actively managed.























































































