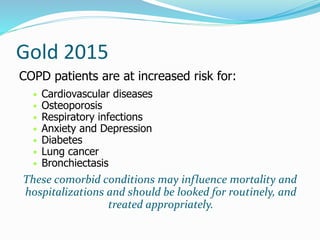
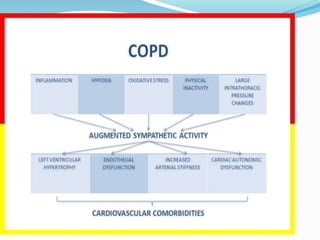
This document discusses systemic inflammation and comorbidities in COPD. It notes that COPD is associated with various important comorbidities beyond the lungs, and inflammation is seen systemically, not just in the lungs. Common comorbidities discussed include cardiovascular diseases like heart disease, hypertension, and stroke. It also mentions increased risk of osteoporosis, diabetes, lung cancer, and other conditions. The systemic inflammation in COPD can be caused by factors like smoking and hypoxia and may contribute to the development and severity of these comorbid conditions.



























































![ Treatment of OSAS does not differ between patients
with COPD and those without.
Treatment of COPD patients with OSAS is based on
the treatment of constituent diseases (for COPD
bronchodilators, inhaled steroids when indicated,
rehabilitation, nutrition, domiciliary oxygen when
indicated, and for OSA weight loss and application of
continuous positive airway pressure [CPAP]).
The goal of treatment is to maintain adequate
oxygenation at all times and to prevent sleep-
disordered breathing.](https://image.slidesharecdn.com/copd-170203141544/85/Copd-68-320.jpg)











































![Copd And The Gold Guidelines 02 21 2005[2]](https://cdn.slidesharecdn.com/ss_thumbnails/copd-and-the-gold-guidelines-022120052-1233826160411176-2-thumbnail.jpg?width=640&height=640&fit=bounds)





















































