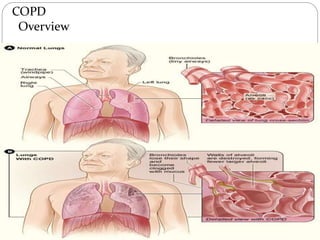
Chronic obstructive pulmonary disease (COPD) is a progressive lung disease characterized by poor airflow. The main causes are smoking and air pollution. Symptoms include cough, sputum production, and shortness of breath. A diagnosis is made through pulmonary function tests showing obstructed airflow. Treatment focuses on smoking cessation, bronchodilators, oxygen therapy, and managing exacerbations.











































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




