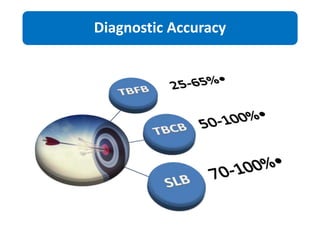
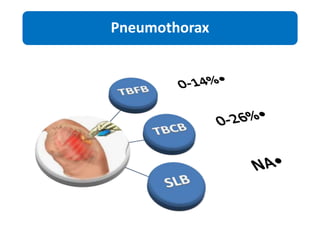
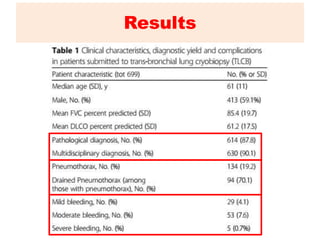
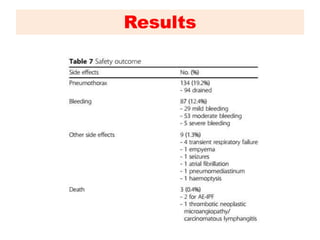
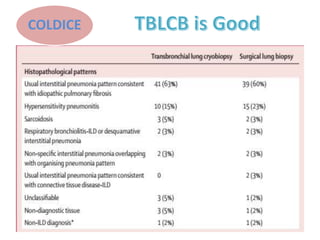
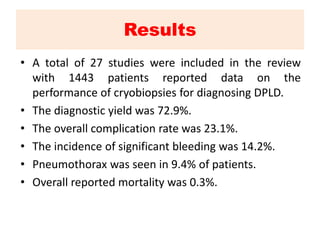
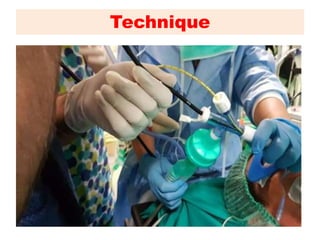



1) Transbronchial cryobiopsy is a bronchoscopic technique that uses extreme cold to obtain biopsy samples and has potential as a safer alternative to surgical lung biopsy for diagnosing interstitial lung diseases. 2) Results from studies show the diagnostic yield of cryobiopsy is around 73% with an overall complication rate of 23%, including pneumothorax in 9.4% of patients and significant bleeding in 14.2%. 3) Guidelines now recommend considering cryobiopsy for suspected idiopathic pulmonary fibrosis when a multidisciplinary team reviews clinical, radiological, and pathological findings.













































































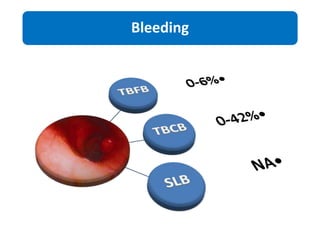
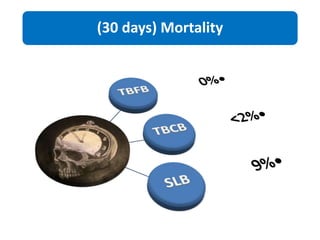
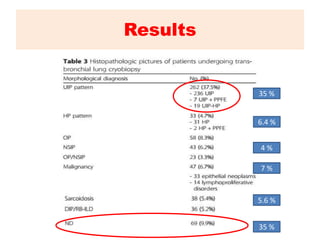
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









