Downloaded 28 times



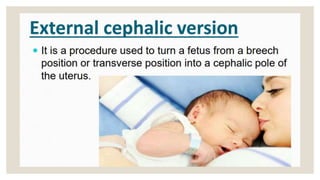
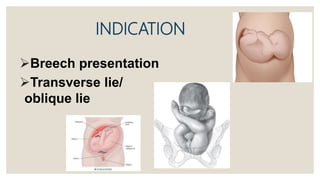
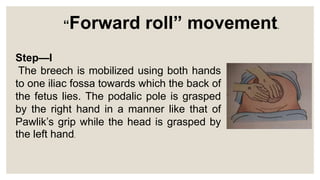
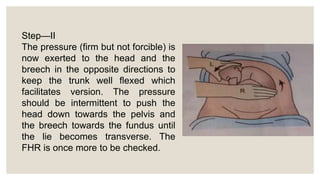


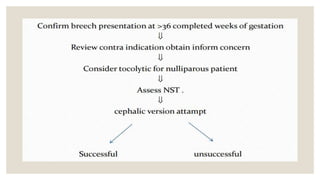


This document discusses unstable lie and version in pregnancy. It defines unstable lie as a condition where the fetal presentation constantly changes beyond 36 weeks of pregnancy when it should have stabilized. Causes include factors that prevent the presenting part from remaining fixed in the lower uterus. Complications include cord entanglement and increased risk of perinatal death. External cephalic version can be attempted to correct the malpresentation if there are no contraindications. Hospitalization is recommended at 37 weeks to monitor for premature rupture of membranes or cord prolapse. Elective c-section is often required, especially if complicating factors are present.










































































