
Recommended
More Related Content
Similar to Obg contracted pelvis and other pelvic deformations
Similar to Obg contracted pelvis and other pelvic deformations (20)
More from Beema3
More from Beema3 (10)
Recently uploaded
Recently uploaded (20)
Obg contracted pelvis and other pelvic deformations
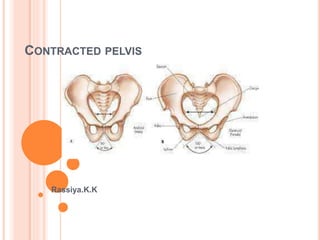
- 2. PELVIS
- 3. Contracted pelvis is an alteration in the size & / shape of the pelvis of sufficient degree so as to alter the normal mechanism of labour in an average size baby.
- 5. Inlet Shortest AP diameter <10 cm Largest transverse diameter <12 cm Midpelvis Interspinous diameter <10 cm Outlet Intertuberous ,, -<8 cm Sub pubic arch narrowing Inter tuberous diameter doesnot admit 4 knuckles.
- 6. Causes 1. Nutritional & environmental Minor variation common Major –Rachitic & osteomalacic 2. Diseases or injuries affecting the pelvis, spine & bones of the lower limbs. Pelvic tumours, Fracture , Tubercular artritis
- 7. Spinal – Kyphosis, Scoliosis, coccygeal deformity. Lower limbs- congenital dislocation of the hip,poliomyelitis in childhood, hip joint disease 3. Developmental defects. Naegle’ pelvis & Robert’s pelvis
- 8. Rachitic pelvis Due to rickets change occure in the soft pelvis due to weight bearing. Sacral promontory is pushed downwards and forwards- shortening AP diameter, sacrum is flat, widening of transverse diameter.
- 10. Osteomalacic pelvis Softening of the pubic bone due to calcium & vit-D deficiency & lack of exposure to sunlight. The promontory is pushed downwards and forwards and the lateral pelvic walls are pushed inwards, anterior wall to form a beak. Approximation of ischeal tuberosities, sacrum shortened and coccyx pushed forward. CS is required.
- 13. Naegle’s pelvis – Arrested development of one ala of the sacrum- may be congenital or aquired as a result of osteitis. Robert’s pelvis. – Ala of both sides are absent & the sacrum is fused with the innominate bones. Transversely contracted pelvis
- 14. NAEGELE’S PELVIS
- 15. ROBERT’S PELVIS
- 16. Scoliotic pelvis.- The body weight fall more on one side of the pelvis than on the other. So the acetabulum is pushed inwards on the weigt bearing side.
- 17. Kyphotic Pelvis. Tilting of upper part of the sacrum backwards&the lower part forwards – increasing AP diameter of inlet & decreasing the same at the outlet.
- 18. DIAGNOSIS OF CONTRACTED PELVIS. Past history – Rickets, osteomalacia, TB of pelvic joints / spine, polio Obstetrical- H/O prolonged & tedious labour followed by Either spontaneous or difficult instrumental delivery. Difficult vaginal delivery ending in still birth/ early neonatal death. Physical examination- Stature- short < 5 ft, any evidence of congenital anomalies- deformity of chest ,spine waddling gait,tilting of the pelvis
- 19. Abdominal examination Inspection- pendulous abdomen specially in primi Non engagement of the head beyond 37 wks in primi malpresentation.
- 20. ASSESSMENT OF PELVIS (PELVIMETRY) Clinical pelvimetry is the assessment of pelvic structures and diameters of pelvis by PV examination. Time- after 37 weeks of gestation , best result when performed after cervical dilatation. Radiopelvimetry Is the use of X-ray in measuring important diameters of pelvis
- 23. Definition The normal proportion between the size of the fetus to the size of the pelvis is disturbed or The disparity in the relation between the head & the pelvis is called CPD. Disproportion may be either due to an average size baby with a small pelvis or due to a big baby with normal size pelvis or due to combination of both.
- 24. Diagnosis. Clinical- Abdominal method, Abdomino vaginal method – Non engagement of fetal head at 38th week in primi. Munro Kerr – Muller method X-ray pelvimetry Cephalometry ( Ultrasonographic measurement of biparietal diameter. MRI
- 25. ABDOMINAL METHOD
- 26. Place pt in dorsal position with thigs slightly flexed and seperated. The head is grasped by the left hand. two fingers ( index and middle) of the right hand are placed above the symphysis pubis with palmar surface of the fingers in line with the anterior surface of the symphysis pubis to note the degree of overlapping if any , when the head is pushed downward downward and back wards.
- 27. Inference - when the head can be pushed down in the pelvis without overlapping of the parietal bone on the SP-no disproportion. -Head can be pushed down a little but there is slight overlapping of the parietal bone evidenced by touch on undersurface of the fingers - moderate disproportion - Head cannot be pushed down and instead the parietal bone overhangs the SP displacing the fingers- severe disproportion.
- 30. Inference - The head can be pushed down upto the level of ischeal spines and there is no overlapping of the parietal bone over the SP - No disproportion The Head can be pushed down a little but not upto the level of ischeal spines and slight overlapping of the parietal bone- slight or moderate disproportion The head can not be pushed down,and the parietal bone overhangs the SP displacing the thumb- Severe dispropotion.
- 33. EFFECTS OF CONTRACTED PELVIS ON PREGNANCY & LABOUR Pregnancy- Incarceration of retroverted gravid uterus in flat pelvis. Pendulous abdomen, malpresentation. Labour- Early rupture ofmembrane , Cordprolapse, slow cervical dilatation, prolonged labour,& in neglected cases obstructed labour with exhaution , dehydration,ketoacidosis & sepsis
- 34. Increased incidence of operative interference, shock, PPH,& sepsis
- 35. MATERNAL INJURIES Cervical tear, vaginal & perineal lacerations In Multigravida increased chance of rupture of the uterus Chance for VVF& RVF Featal Hazards Trauma & Asphyxia
- 36. MANAGEMENT OF CONTRACTED PELVIS ( INLET CONTRACTION) Premature induction of labour Elective CS at term Trial labour.
- 37. PREMATURE INDUCTION Induction 2-3 weeks prior to due date , the size of the baby is smaller, so that spontaneous vaginal delivery is possible Elective CS at term Indication Major degree of inlet contraction Moderate degree of inlet contraction with outlet contraction or with complicating factors.
- 38. TRIAL LABOUR Is the conduction of spontaneous labour in a moderate degree of cephalo pelvic disproportion,in an institution under supervision with watchful expectancy, hoping for a vaginal delivery. Aims Avoiding unnecessary CS & delivering a living undamaged child
- 39. Contra indication * Associated midpelvic & outlet contraction * Presence of complicating factors – elderly primi, GDM, PIH, malpresentation Post CS * Unfavourable surroundings
- 40. CONDUCTION OF TRIAL LABOUR Labour should ideally spontaneous onset Prevent early rupture of membrane- enema should not be given & the pt should be in bed. Keep NPO status ,IV glucose drip, I/O chart Analgesics Partogram If there is no progress ,Induction of labour by LROM followed by oxytocin drip
- 41. PV examination to exclude cord prolapse, colour of liqour,
- 42. Duration of trial labour As long as the membranes are intact ,Progress is satisfactory,& maternal &fetal condition remain good trial may be continued. Not to wait for more than half an hr after the ROM with Cx fully dilated.
- 43. Unfavourable Features. Abnormal uterine contraction Early ROM Postr Presentation Cervical dilatation <1 cm /hr with good uterine contractions. Thick & edematous Cx Formation of caput & evidence s of moulding Fetal distress.
- 44. TERMINATION OF TRIAL LABOUR Spontaneous labour ( 30%) Forceps or ventous ( 30%) CS ( 40%)
- 45. Successful Trial:- if an damaged baby is born vaginally, spontaneously or by forceps or ventous with the mother in good condition. Delivery by CS or delivery of a dead baby spontaneously or by craniotomy – Failure of trial labour
- 46. Advantages * Eliminate unnecessary CS * A successful trial gives guarantee to her future obstetrics. Disadvantages * Increased perinatal mortality * Increased Maternal morbidity