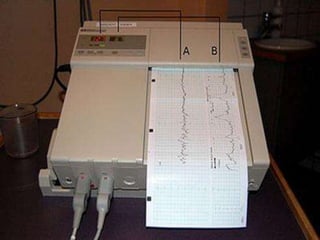
The non-stress test (NST) is a common prenatal test used to evaluate fetal well-being in the third trimester of pregnancy. The test involves continuous electronic monitoring of the fetal heart rate and movements using ultrasound or other sensors. It is a non-invasive test performed when the fetus is over 28 weeks of gestation. During the 20-40 minute test, accelerations in the fetal heart rate in response to movement are evaluated to determine if the fetus is reactive and healthy or non-reactive, which may require further evaluation. The test helps assess fetal oxygen levels and growth without placing stress on the fetus.







































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)










