Download to read offline

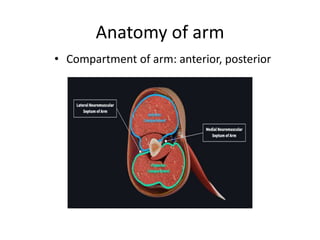






























































This document provides an overview of compartment syndrome, including: - The anatomy of the arm, forearm, hand, thigh, leg, and foot compartments. - The causes, signs/symptoms, and diagnostic criteria for acute compartment syndrome. Tissue damage can become irreversible after 6-8 hours of increased compartment pressure. - Surgical fasciotomy is required if increased compartment pressure does not improve with simple measures like removing external compression. Complete release of all compartments is needed. - Post-operative wound management includes wet-to-dry dressing changes or negative pressure wound therapy to promote healing and prevent infection following fasciotomy.























































