Downloaded 15 times
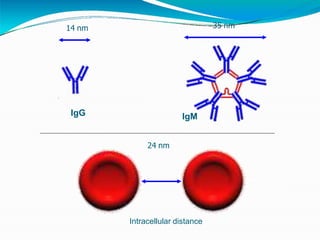
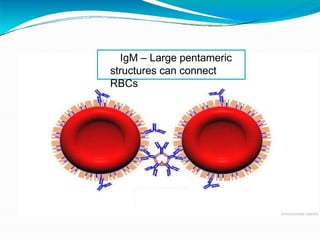
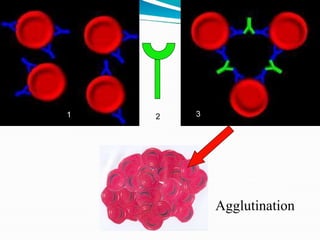
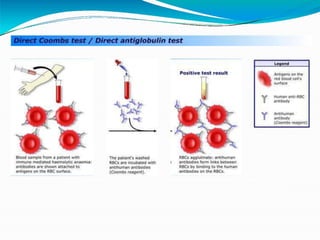
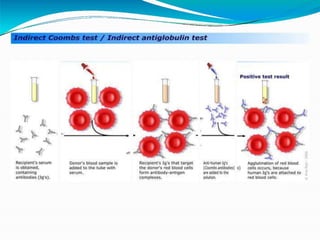
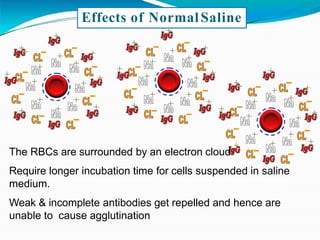
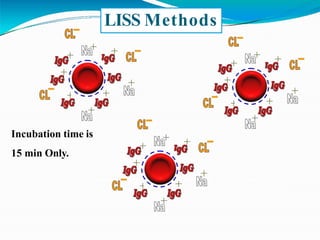






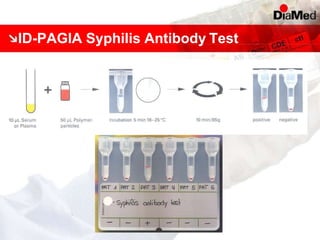









This document discusses gel technology used in blood banking and immunohaematology. It provides historical aspects of blood banking, basics of immunohaematology, principles of gel technology, grading of reactions, applications including blood grouping, antibody screening and identification, cross matching, and direct and indirect antiglobulin tests. It discusses the advantages of gel technology including improved sensitivity and specificity, ease of use, reliable and reproducible results. Literature on using gel technology for compatibility testing, diagnosis of autoimmune hemolytic anemia, and its increased sensitivity over conventional tube technique is also reviewed.



































































