Download to read offline
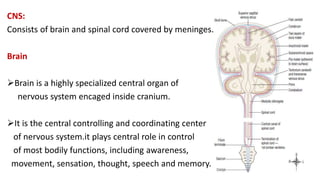
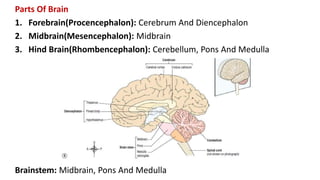






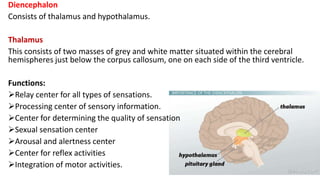


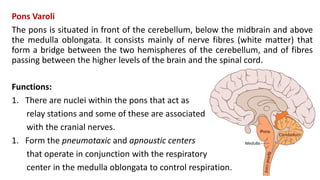
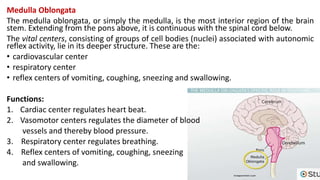


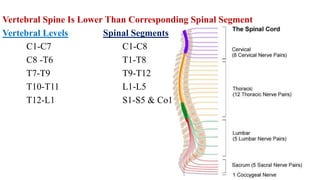



















The central nervous system consists of the brain and spinal cord, which are covered by three layers of meninges. The brain is divided into the forebrain, midbrain, and hindbrain. The forebrain includes the cerebrum and diencephalon. The cerebrum is made up of four lobes that control functions like movement, sensation, thought, and memory. The diencephalon contains the thalamus and hypothalamus, which relay sensory information and control autonomic functions respectively. The midbrain relays information between the brain and spinal cord. The hindbrain contains the cerebellum, pons, and medulla, which coordinate movement, relay information, and control vital functions. The spinal























































































