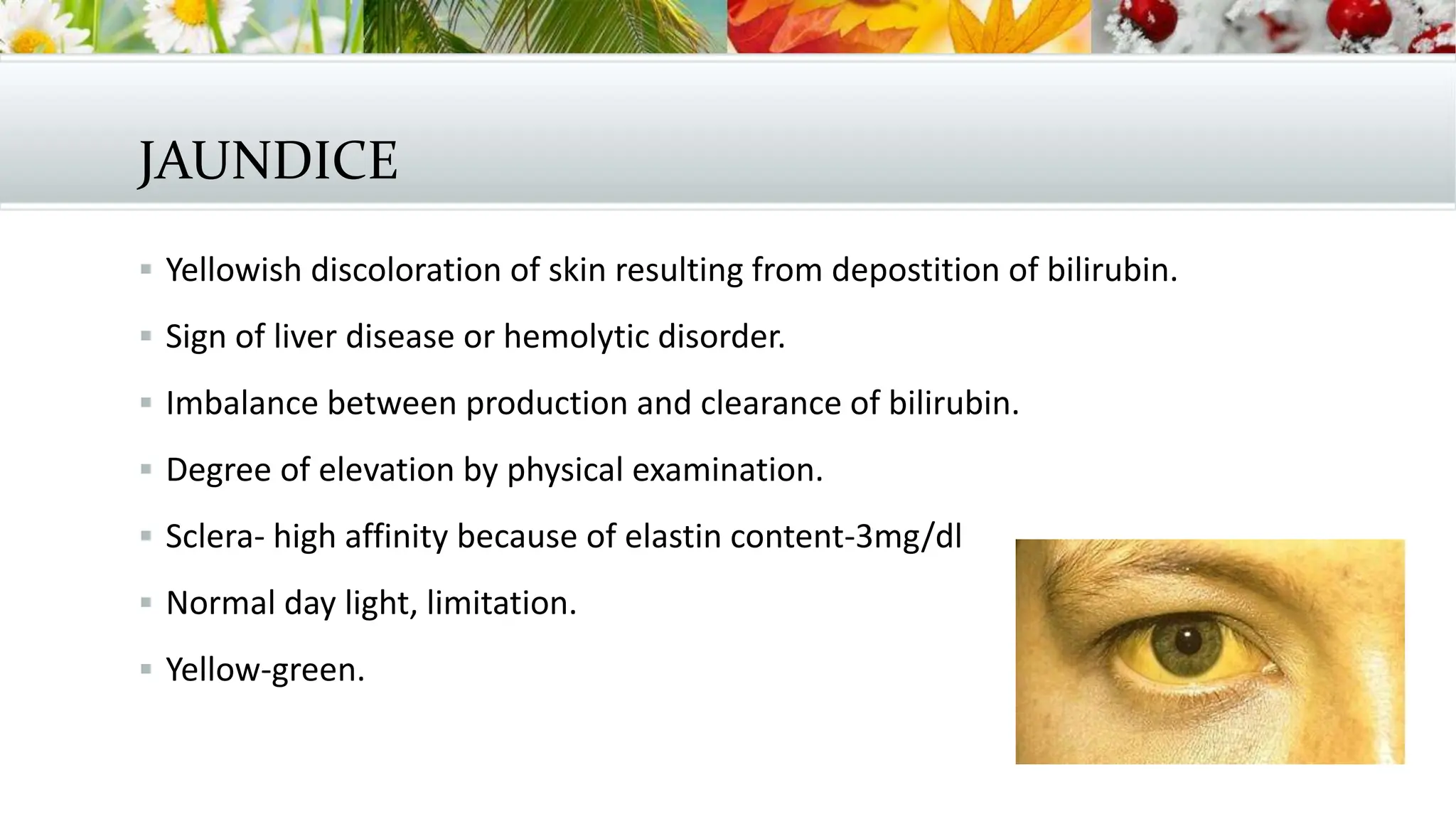
This document provides an overview of the clinical approach to jaundice. It discusses the production and metabolism of bilirubin, measurement of bilirubin levels, causes of hyperbilirubinemia including hepatic and extrahepatic sources, and the approach to evaluating a patient with jaundice through history, physical exam, and laboratory tests. Common etiologies like viral hepatitis, drug toxicity, and biliary obstruction are reviewed. A thorough workup is needed to determine if the source of jaundice is from overproduction, impaired clearance, or obstruction of bilirubin.