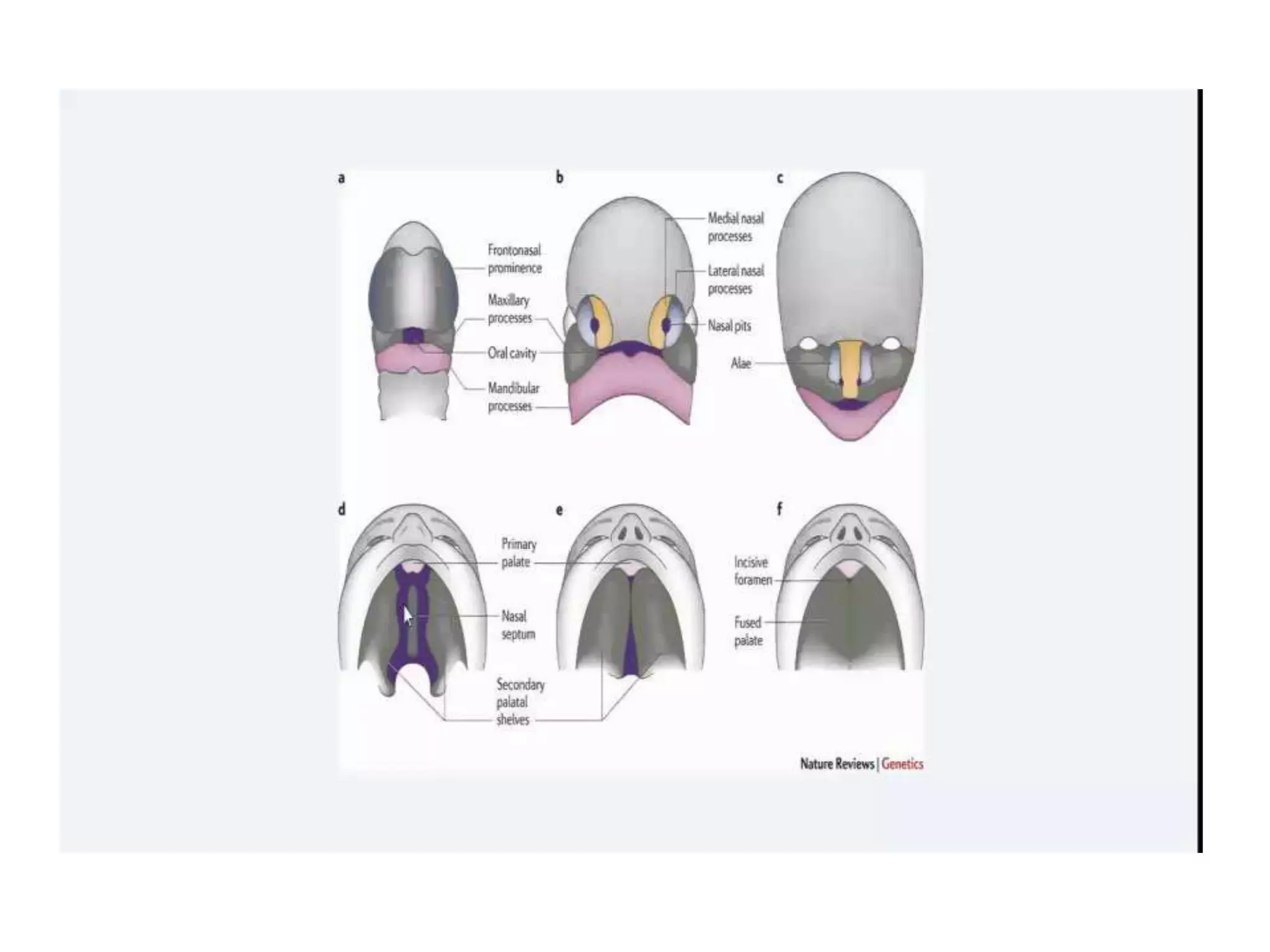
This document discusses cleft lip and palate including embryogenesis, classification systems, incidence, etiology, management, and timing of surgery. It describes how the lip and palate form during embryogenesis. It covers several classification systems including Nagpur, LAHSHAL, Davis & Ritchie, and Veau systems. It provides statistics on incidence. It discusses etiology such as familial factors, nutrition, infections, radiation, and genetic syndromes. It outlines primary and secondary management including feeding, airway, surgery, and secondary concerns like hearing, speech, dental issues, and potential additional surgeries.