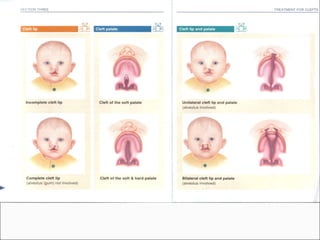
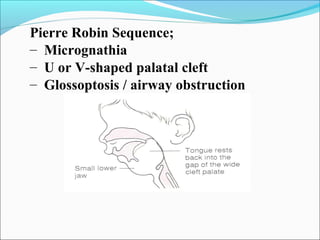
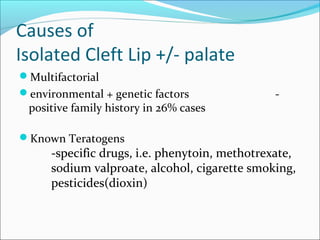
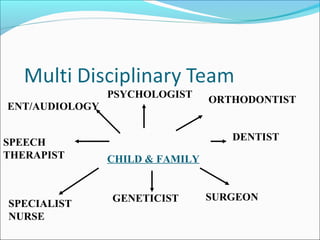
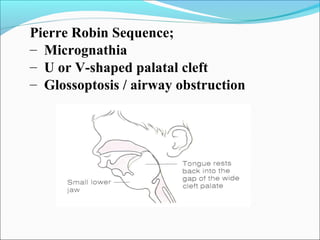
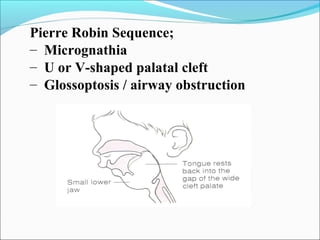
Pierre Robin sequence involves micrognathia, a cleft palate, and airway obstruction. Cleft lip and palate can be caused by genetic and environmental factors. Feeding difficulties are common in infants with clefts due to issues creating suction and maintaining nipple contact. A multidisciplinary team supports families throughout treatment including surgery, speech therapy, and orthodontics from infancy through adulthood.