Downloaded 331 times
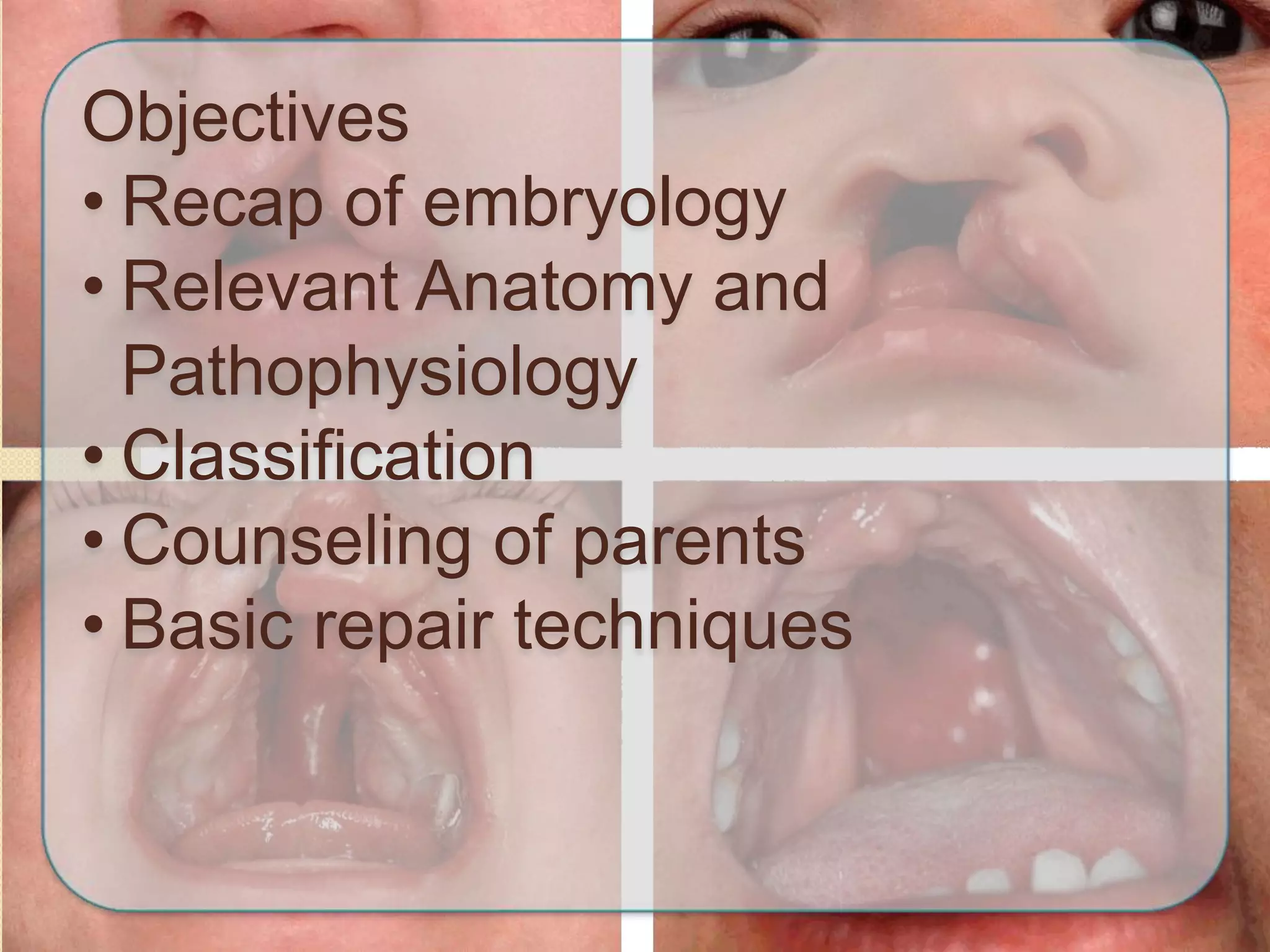
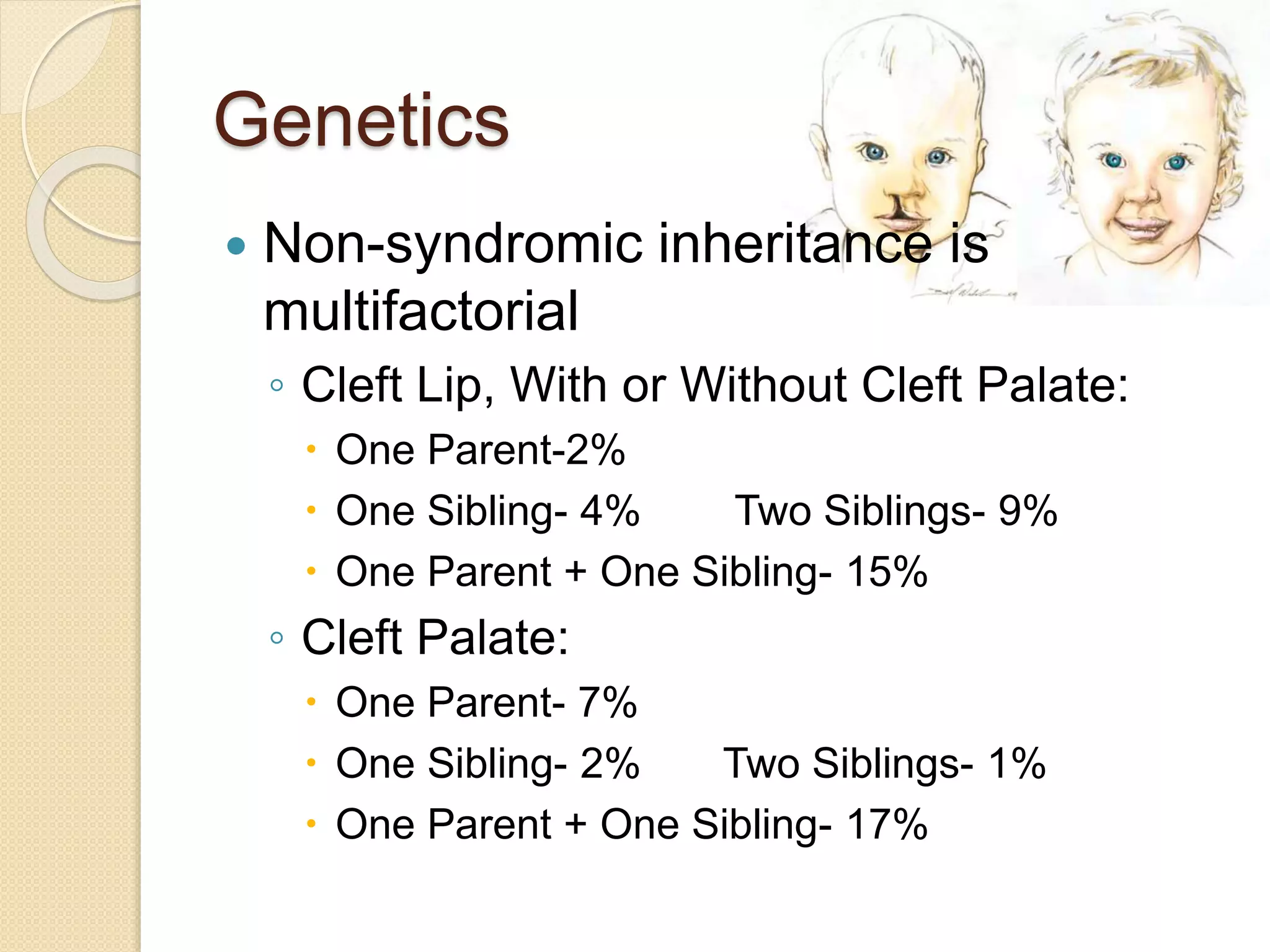
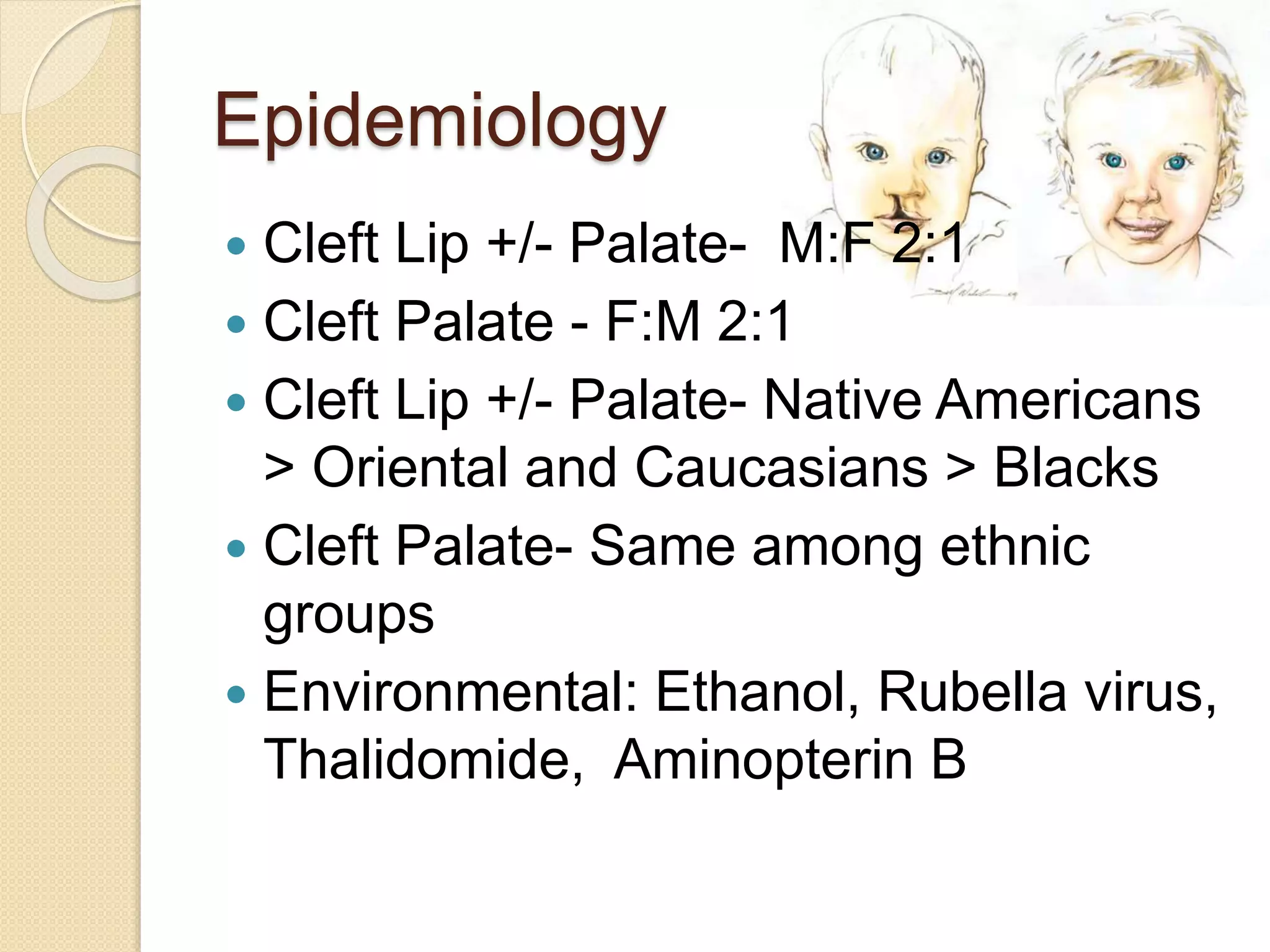
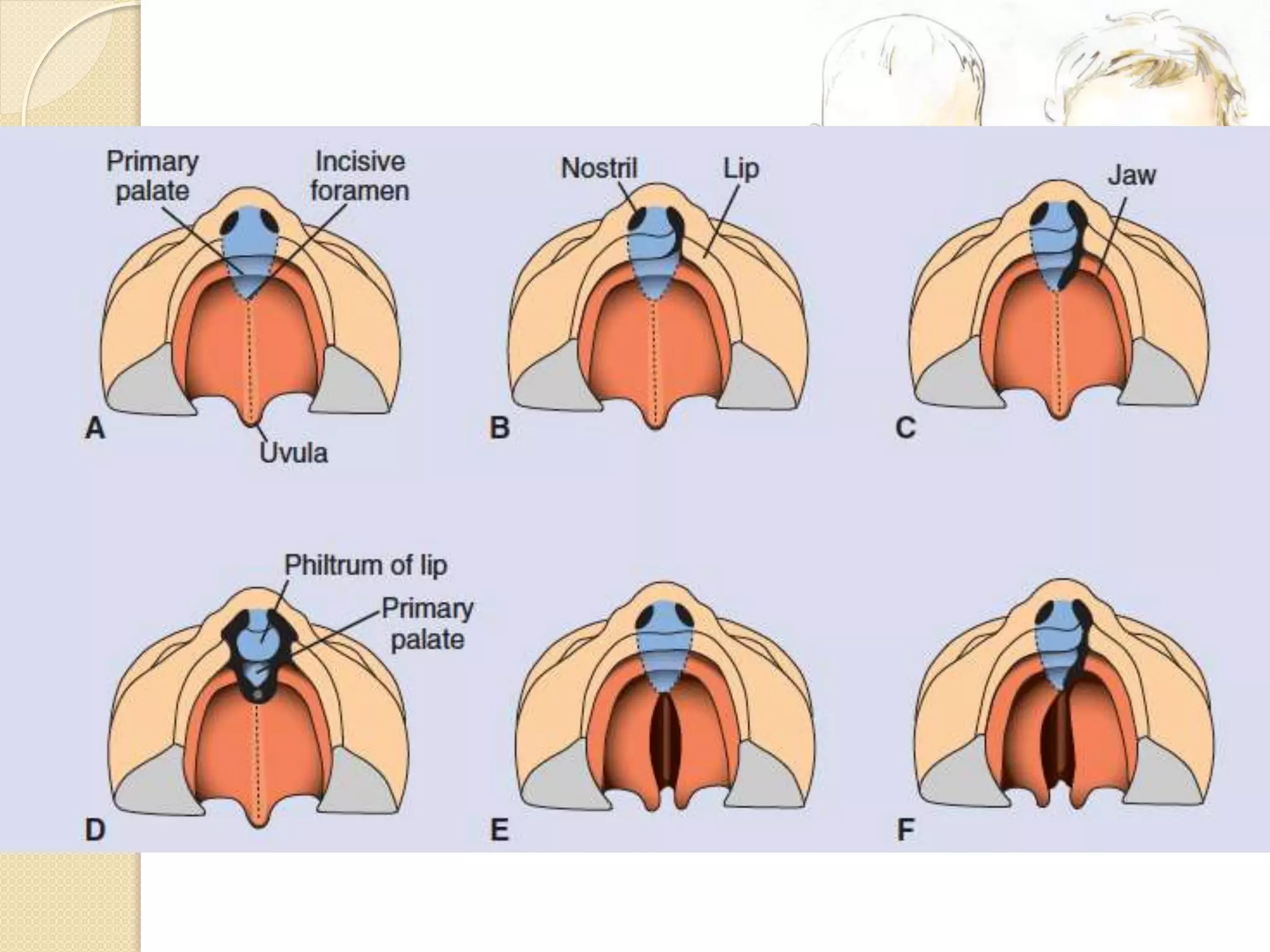
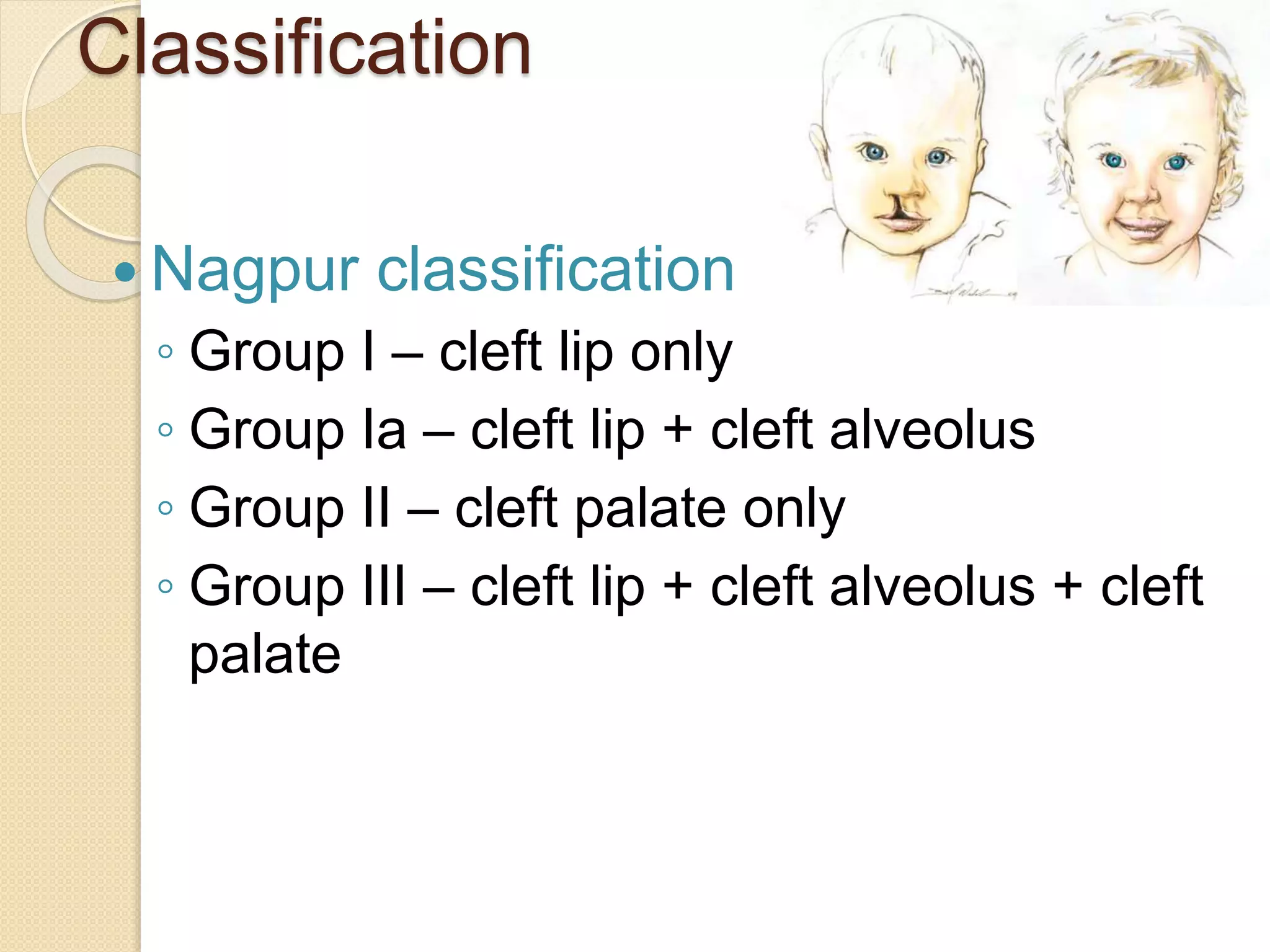
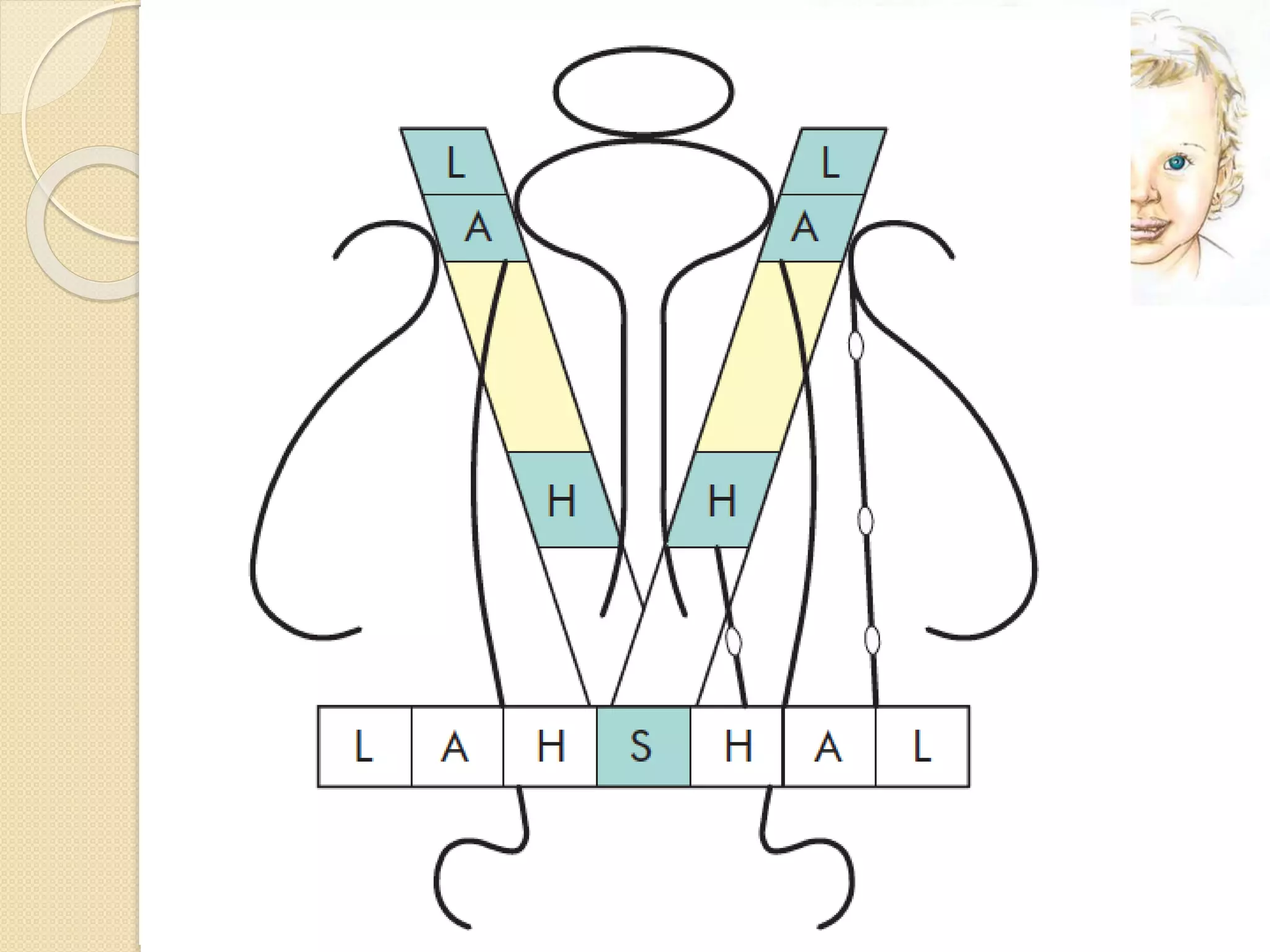




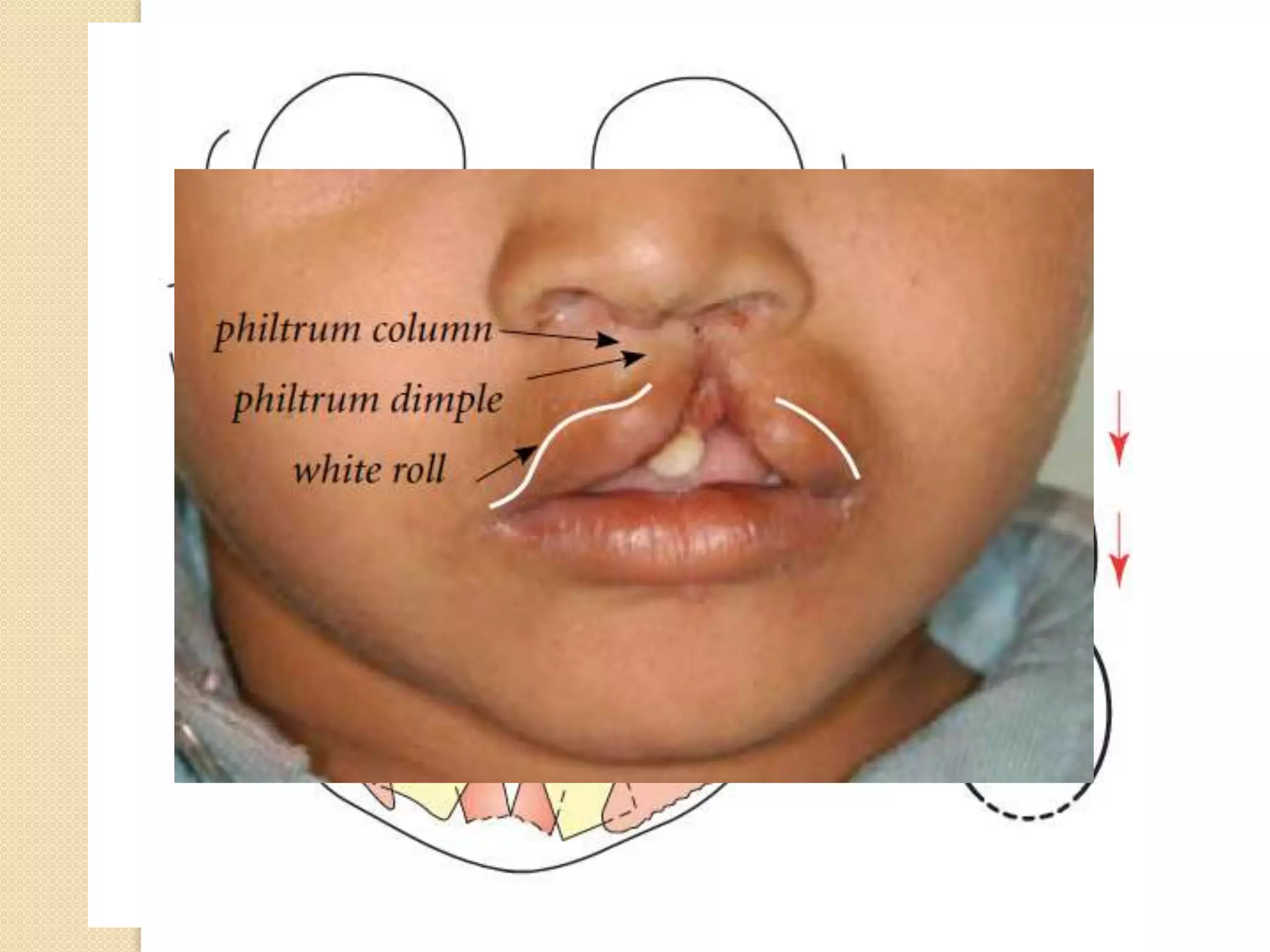

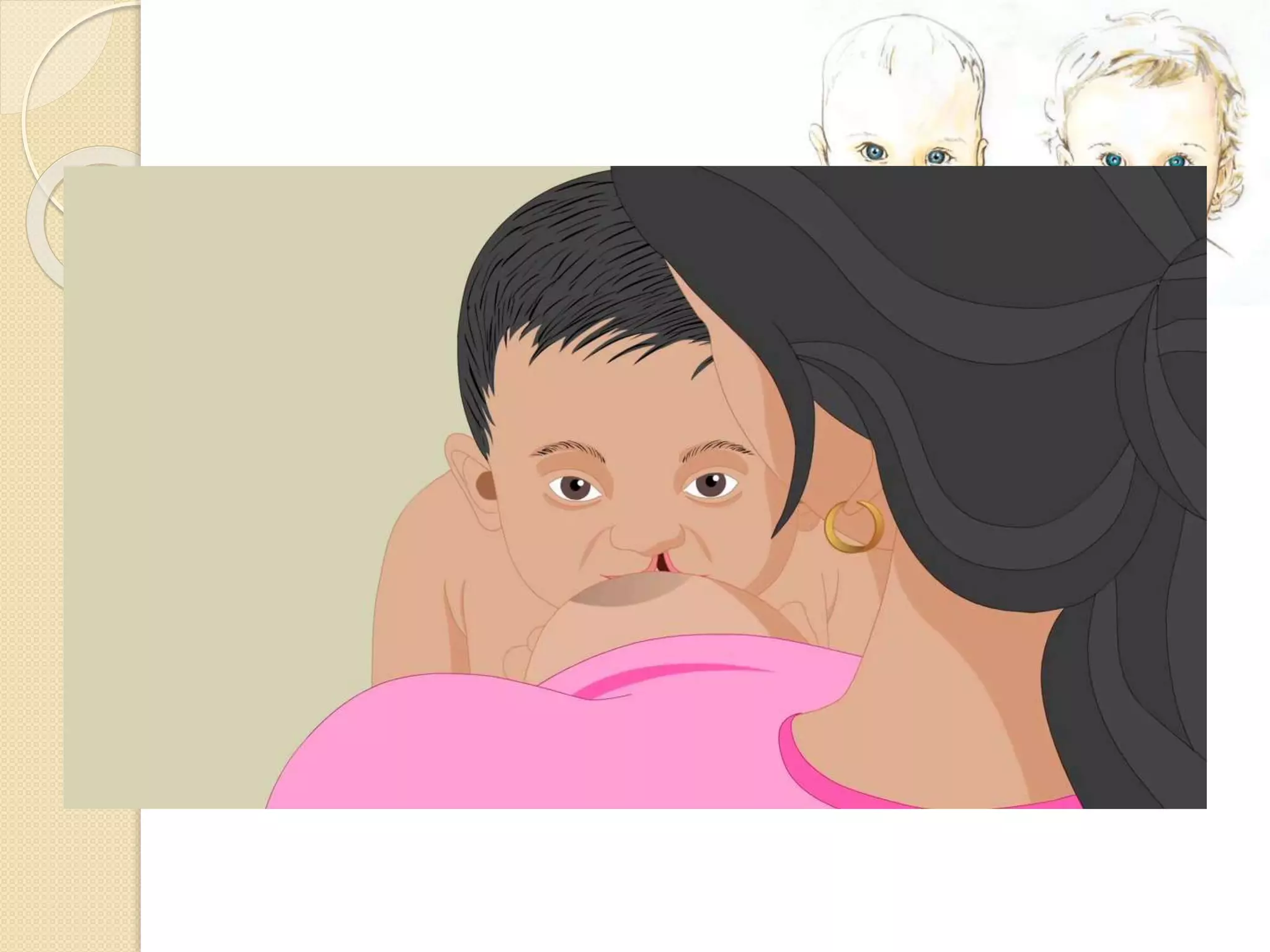


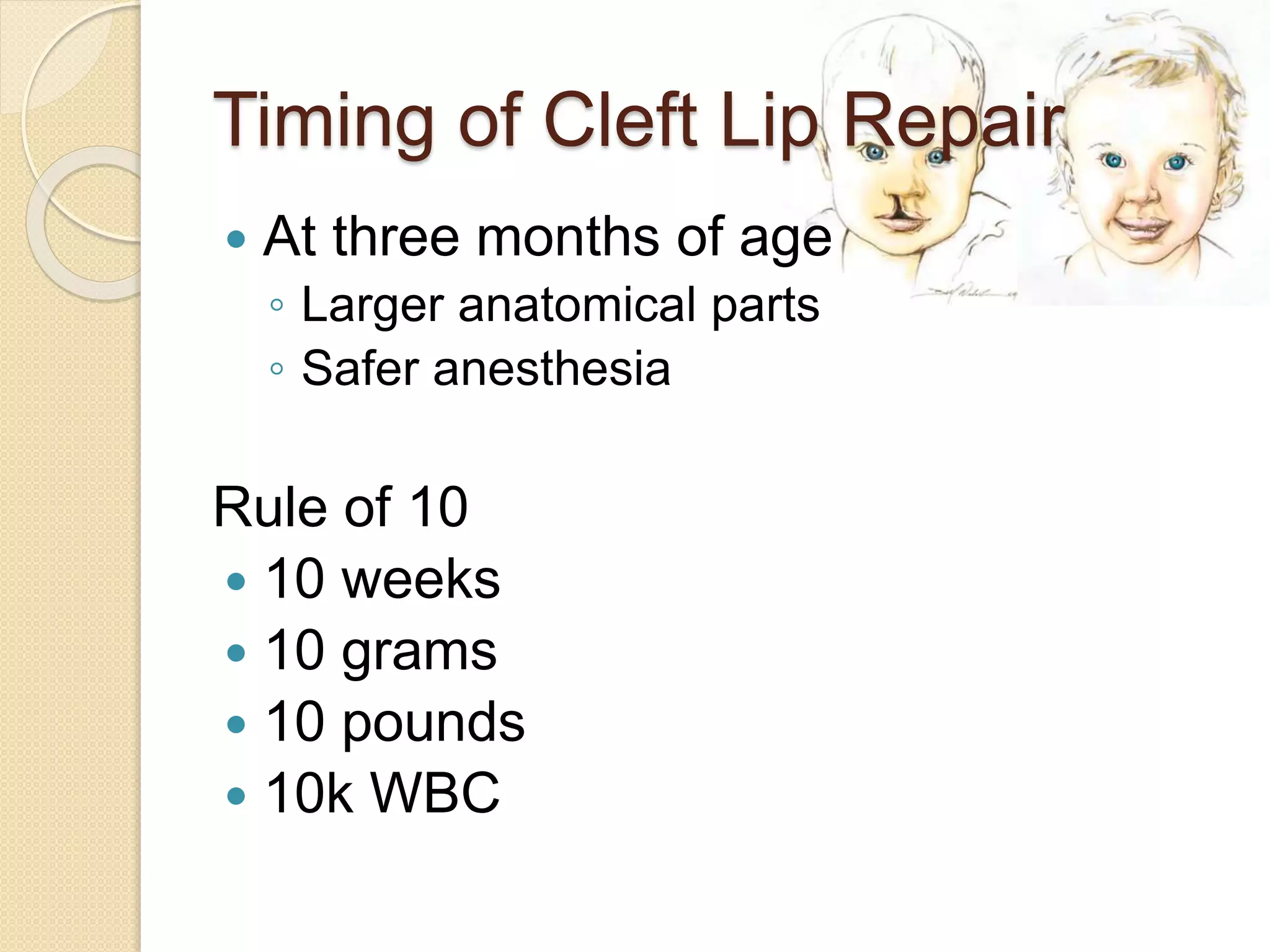
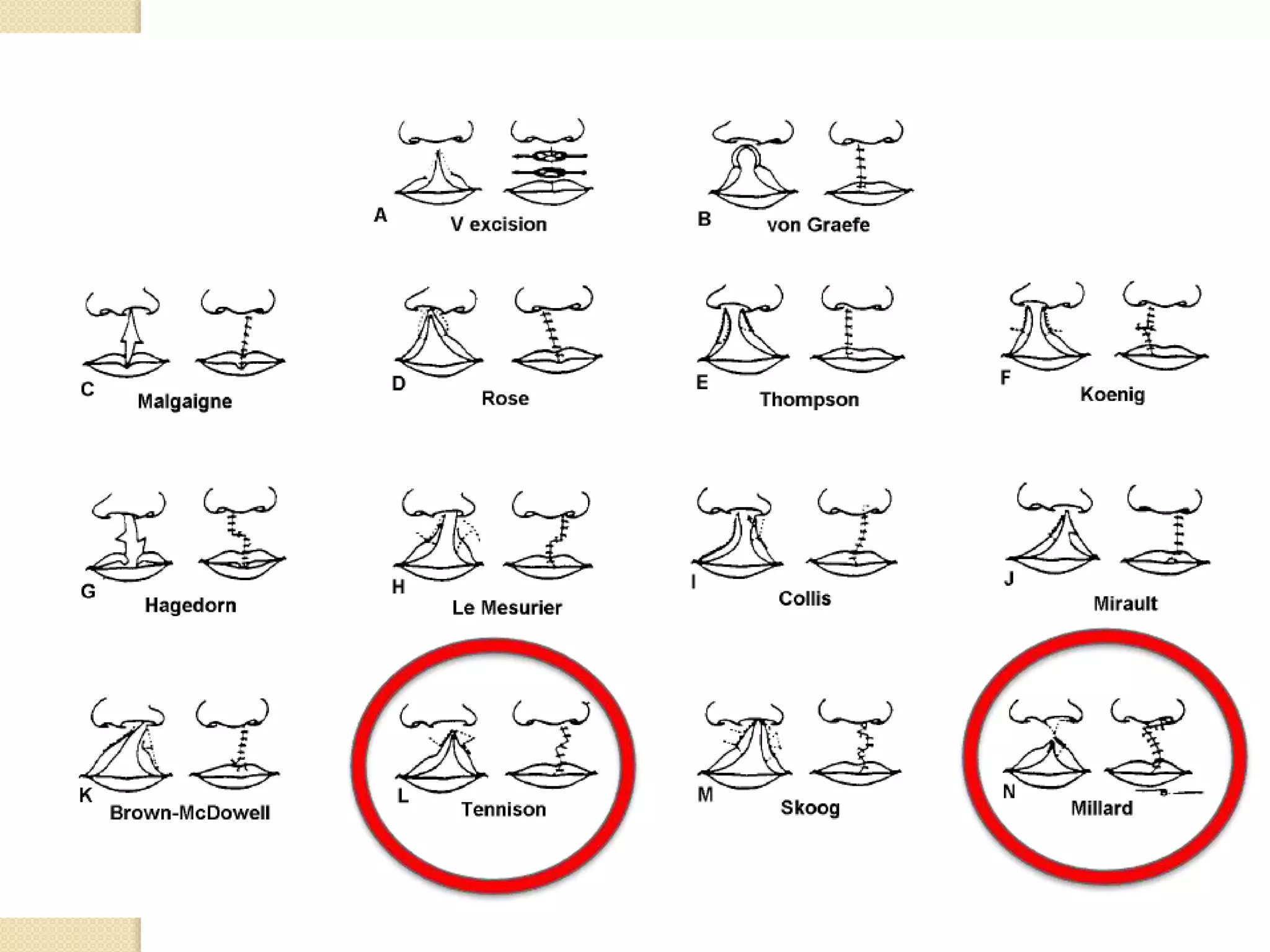
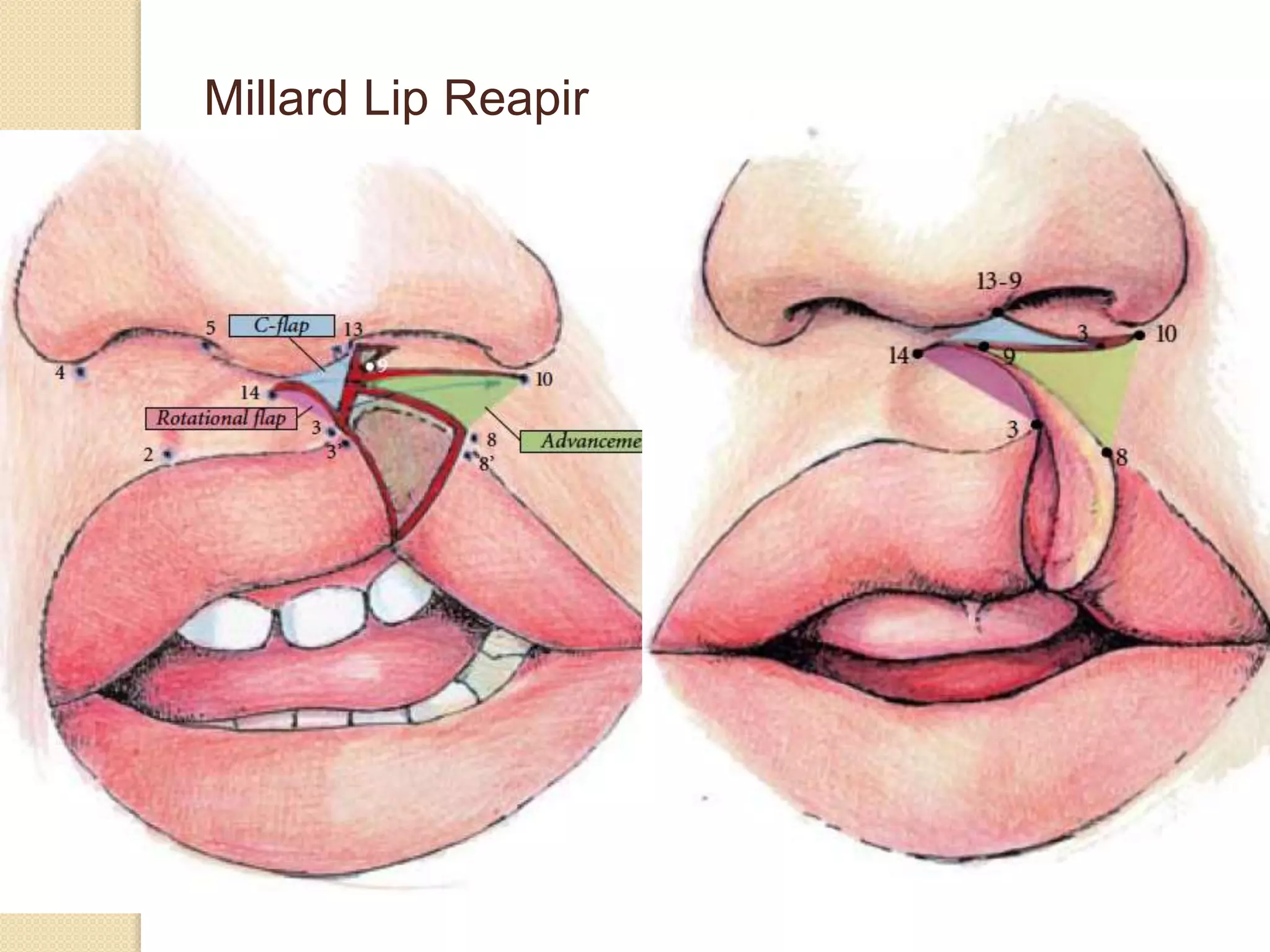
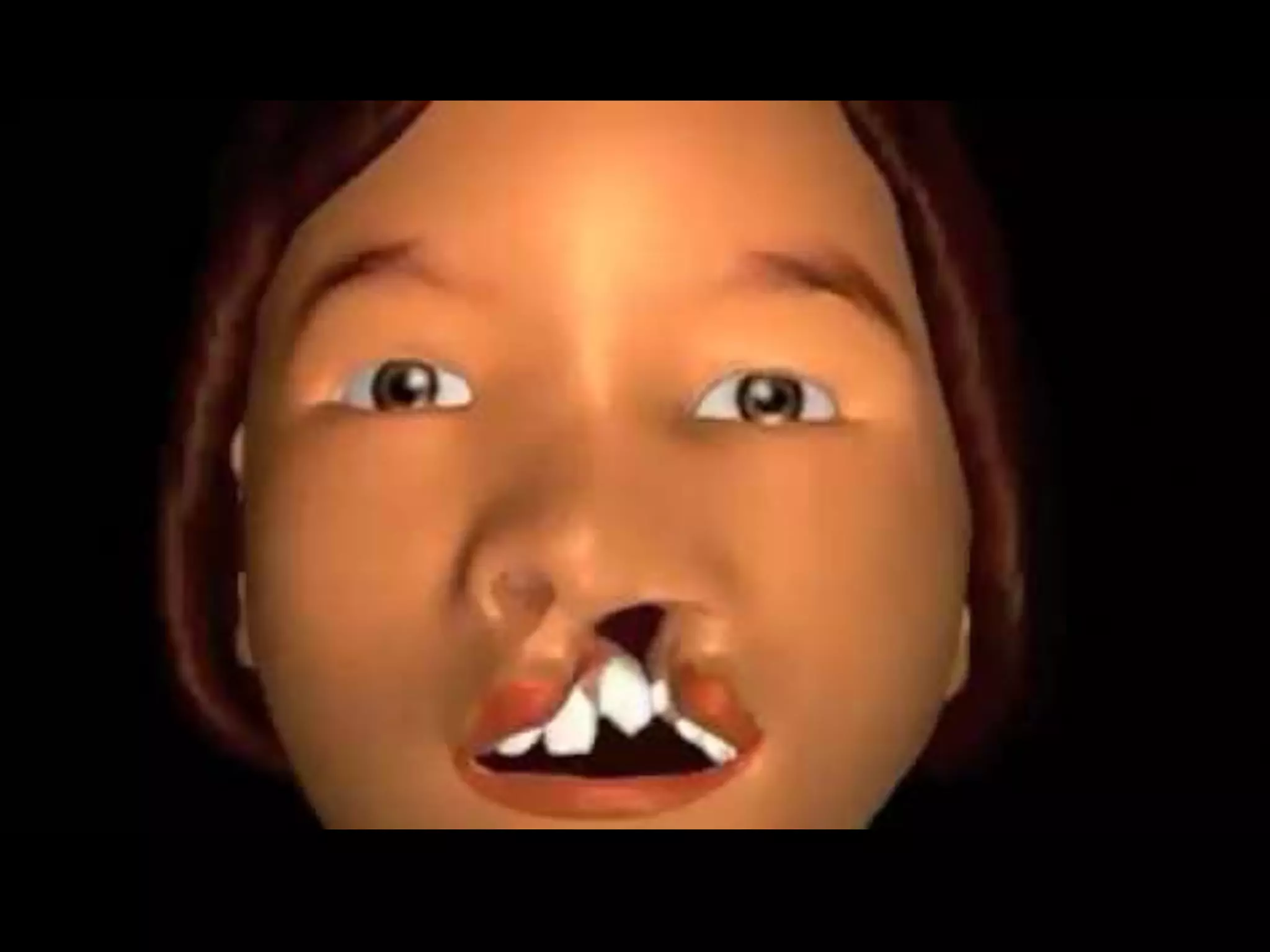
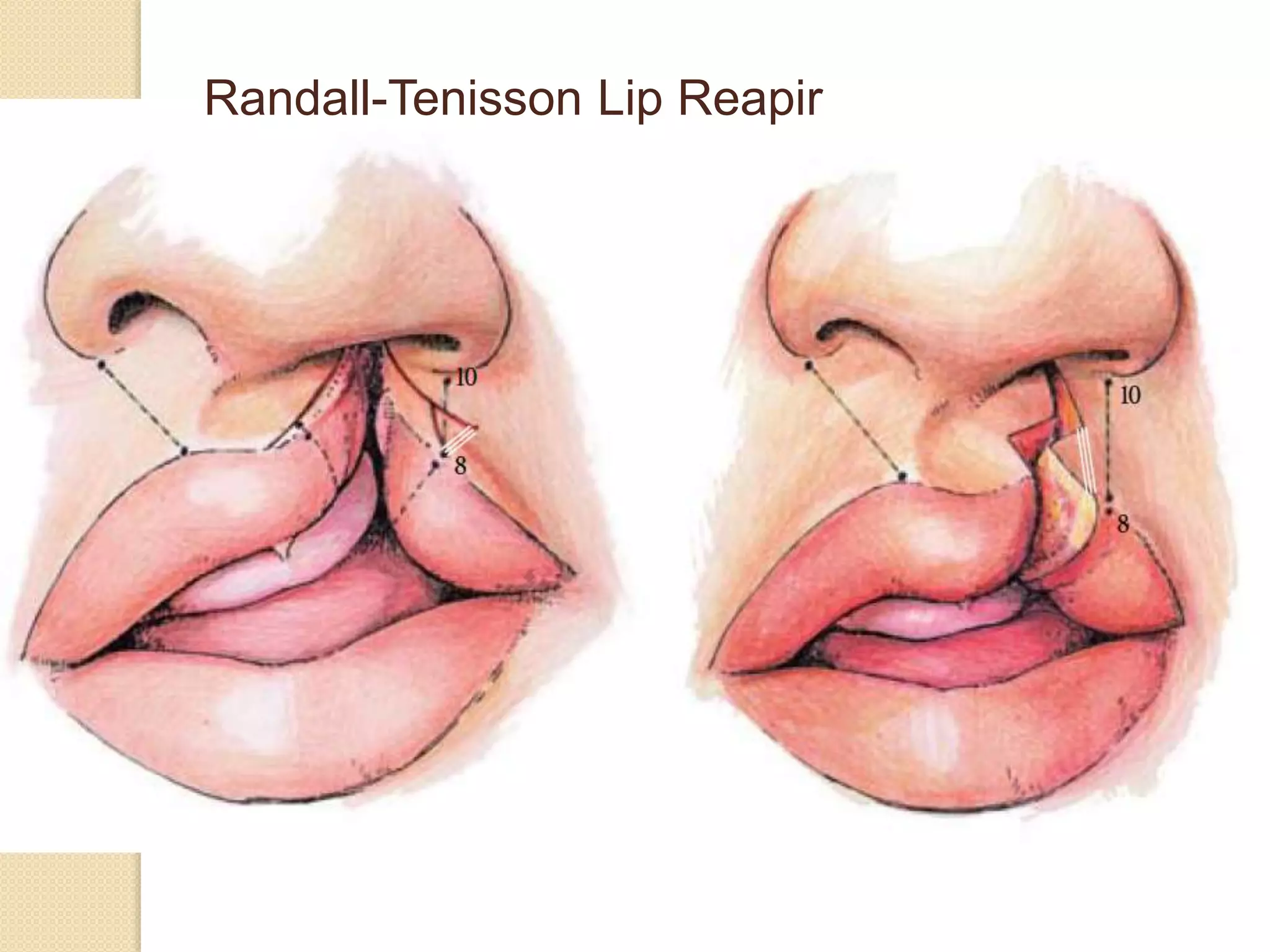
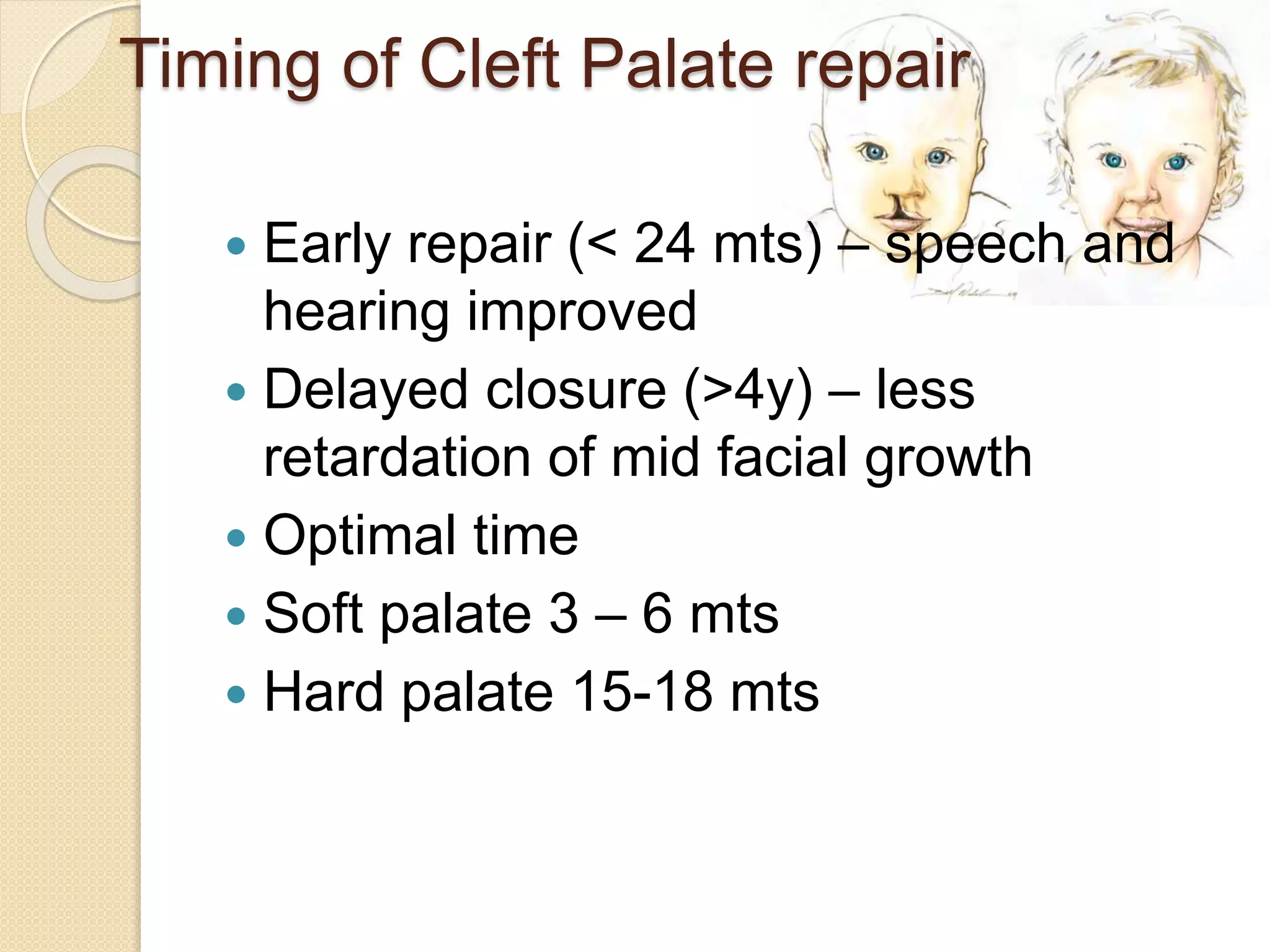
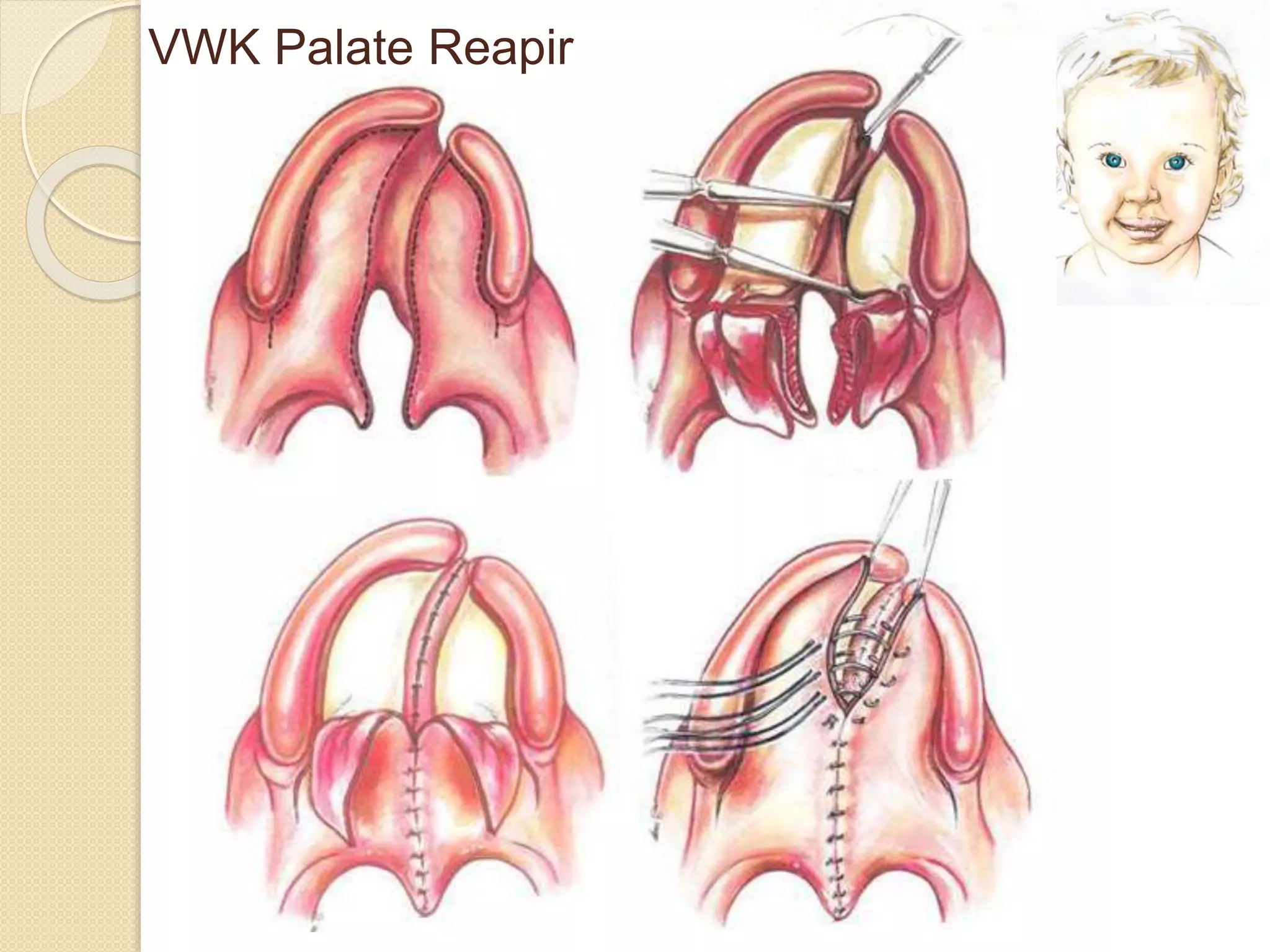
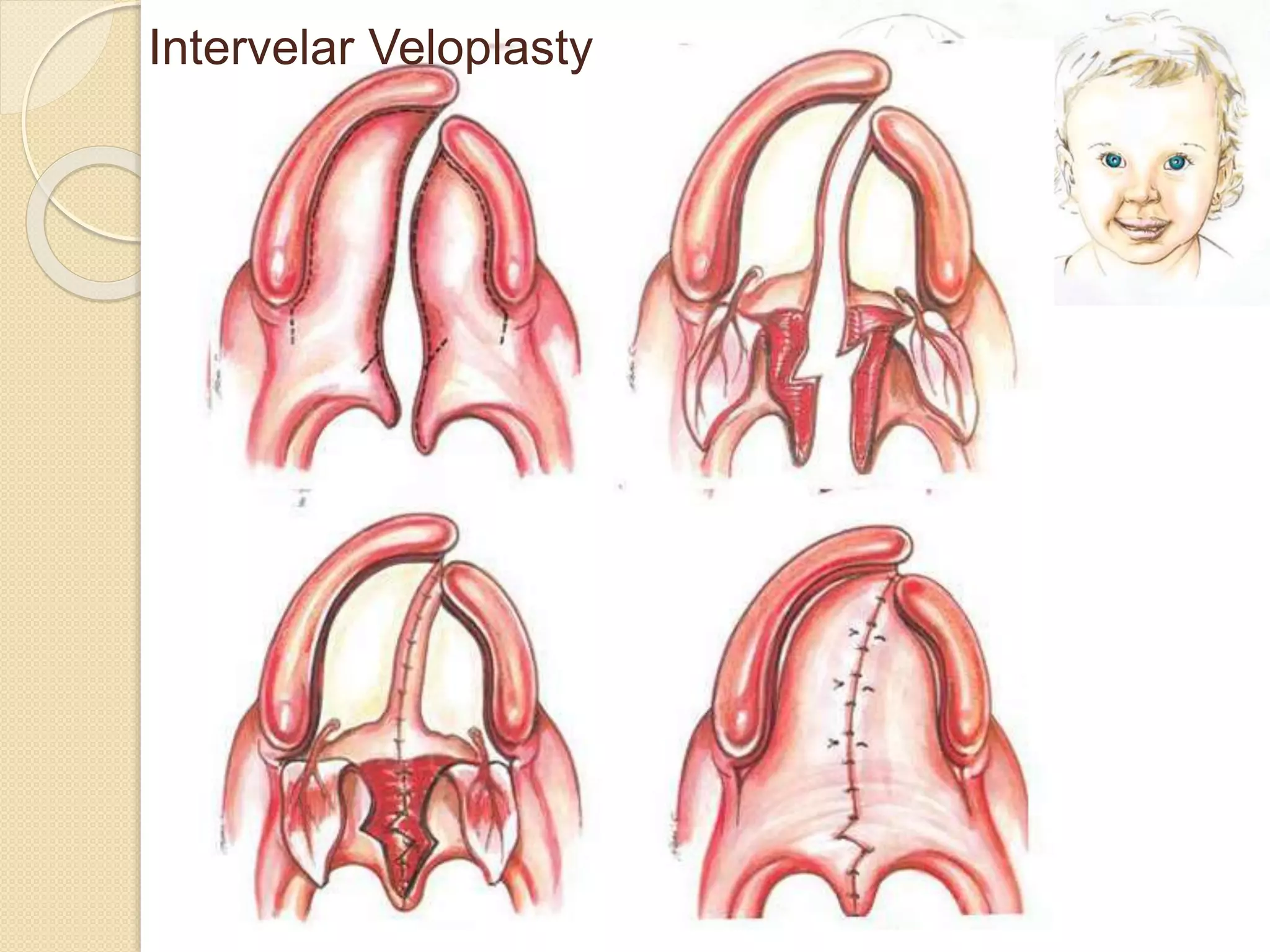
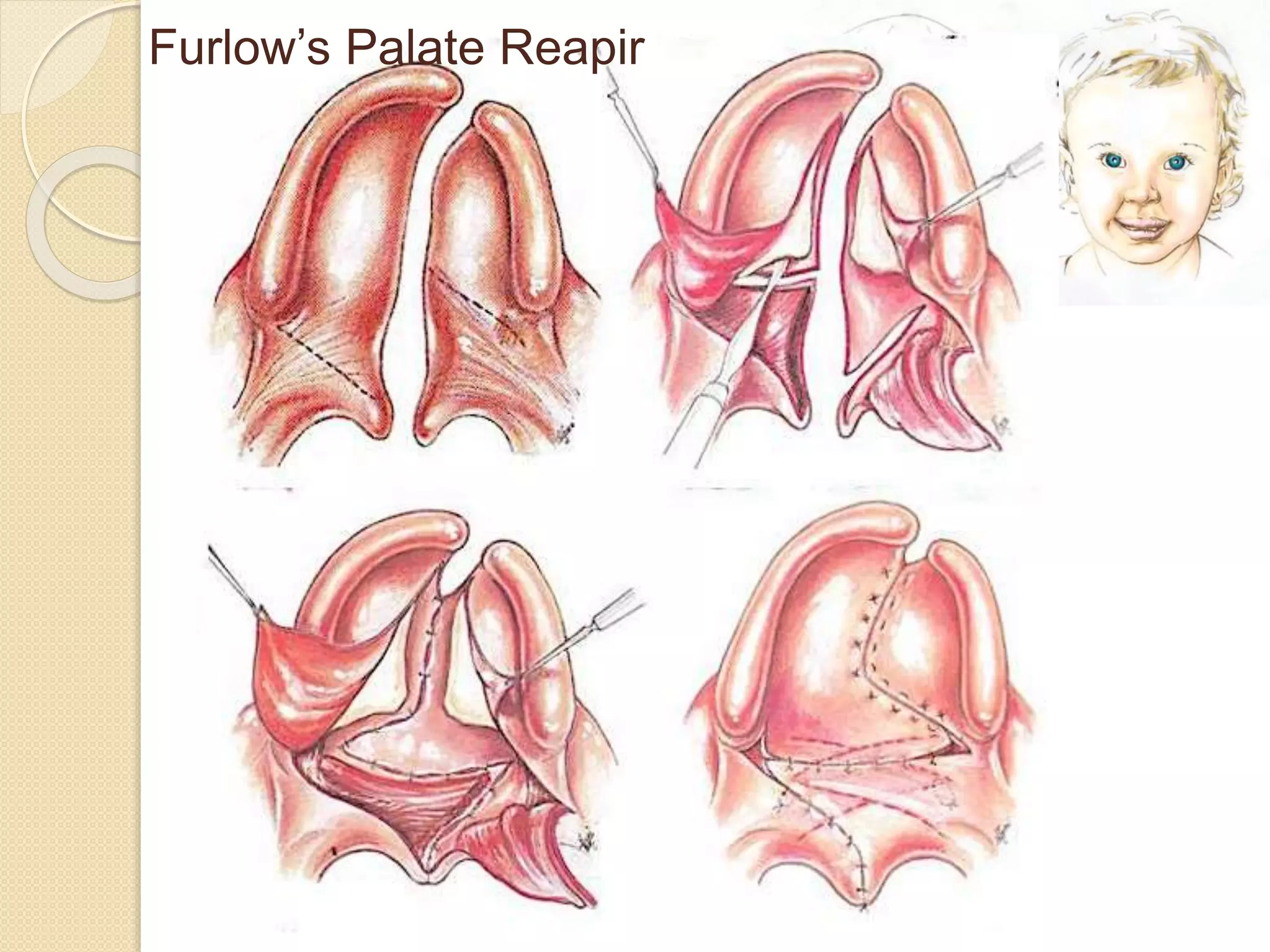
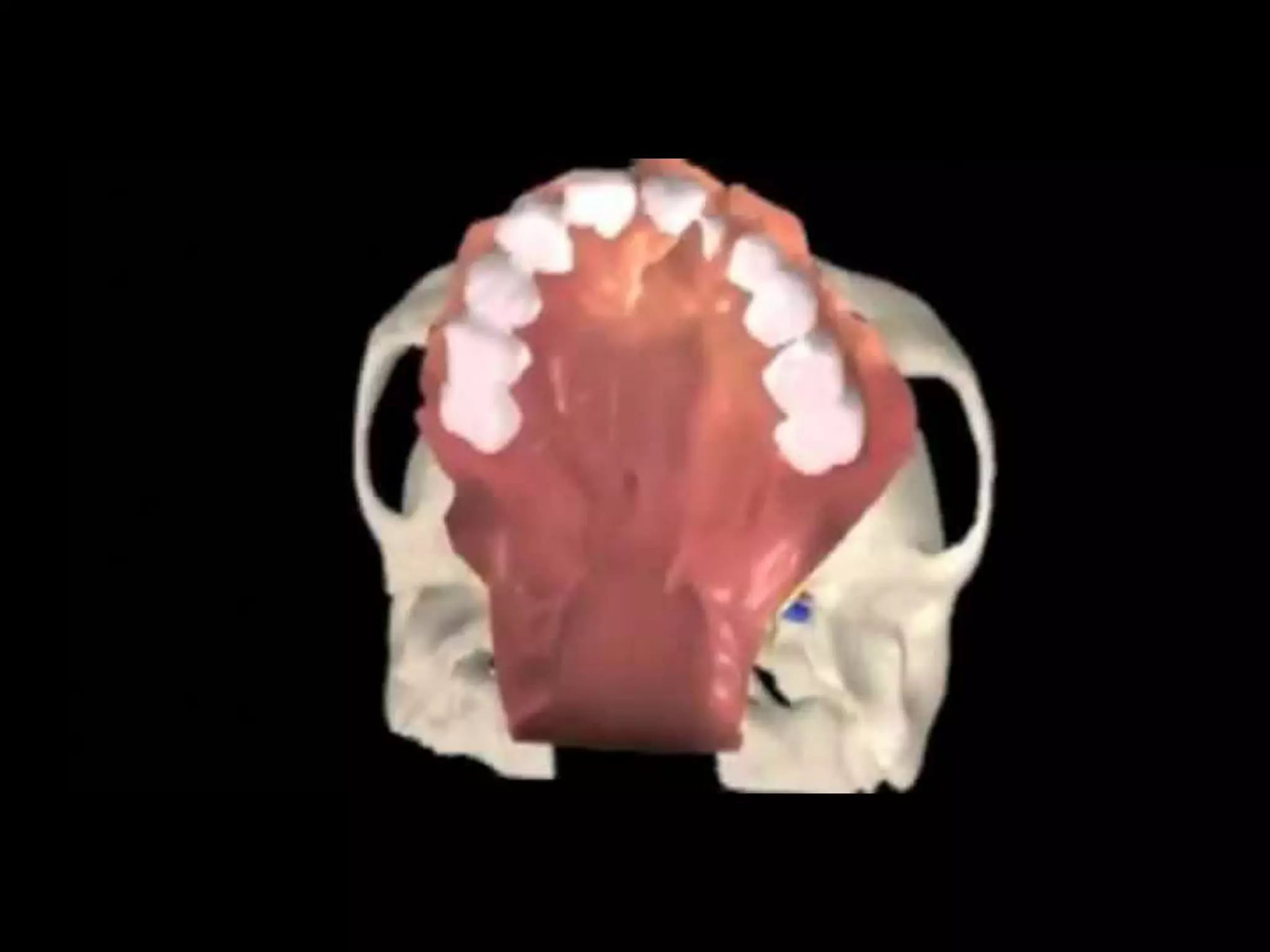

This document discusses cleft lip and palate, including the relevant anatomy, pathophysiology, classification, and surgical repair techniques. Cleft lip and/or palate is the second most common birth defect, affecting speech, feeding, hearing, and emotional development. The causes are multifactorial, with both genetic and environmental factors playing a role. Surgical repair of cleft lip is typically done at 3 months of age, while cleft palate repair is usually between 3-6 months for the soft palate and 15-18 months for the hard palate. The document reviews several techniques for cleft lip and palate repair, as well as complications to watch for. It emphasizes the importance of a multidisciplinary



































































