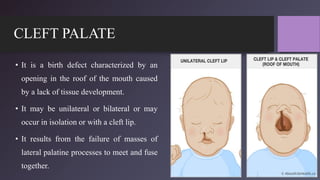
The document discusses the management of children with cleft lip and palate, outlining the embryology, classification, incidence, etiology, clinical features, and problems associated with these congenital malformations. It emphasizes the need for a multi-disciplinary approach for diagnosis and treatment, including various surgical procedures and nursing management strategies. Additionally, it details the practical nursing interventions required to address nutritional needs, respiratory issues, and parental anxiety related to the condition.