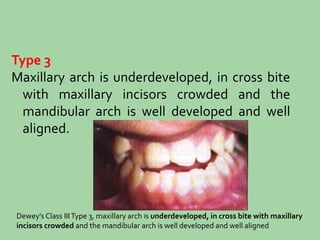
This document provides an overview of various classifications of malocclusion. It begins by dividing malocclusions into three broad categories: individual tooth malpositions, malrelation of dental arches, and skeletal malocclusions. It then discusses Angle's classification system in detail, which divides malocclusions into Classes I, II, and III based on the relationship of the maxillary and mandibular first molars. The document also discusses modifications to Angle's classification by Dewey and others. It provides examples to illustrate different types of individual tooth malpositions, arch malrelations, and skeletal malocclusions.



































![Classification_of_malocclusion[1] [Read-Only].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/classificationofmalocclusion1read-only-240212164016-9b5c21cb-thumbnail.jpg?width=640&height=640&fit=bounds)











































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)












