Downloaded 13 times




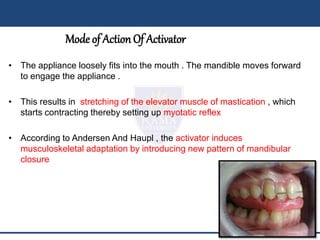
































The document discusses the history and development of the activator appliance. Some key points: - The activator was developed in the late 1800s as a modification of earlier appliances to guide mandibular positioning. - It uses light forces and proprioceptive stimulation to encourage favorable jaw growth. - Taking an accurate construction bite to determine vertical and horizontal displacement is important for fabrication. - The activator is trimmed over time to guide tooth eruption into the desired occlusion. - It is indicated for Class II and III malocclusions in growing individuals, and various modifications have been developed.


































![---Activator and its modifications[14.9.16=8.29 pm]](https://cdn.slidesharecdn.com/ss_thumbnails/activatoranditsmodifications14-160916143340-thumbnail.jpg?width=640&height=640&fit=bounds)
























