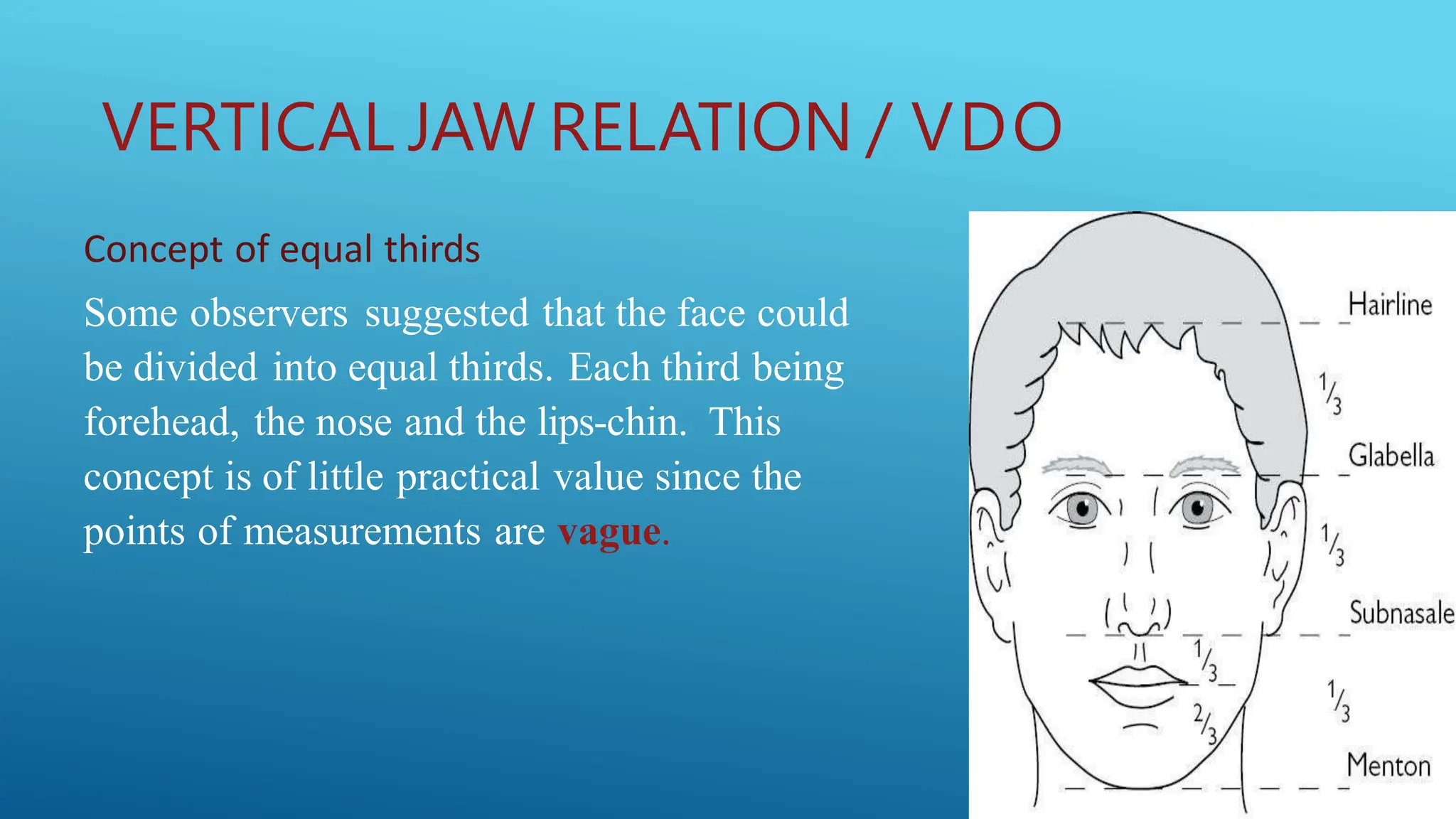
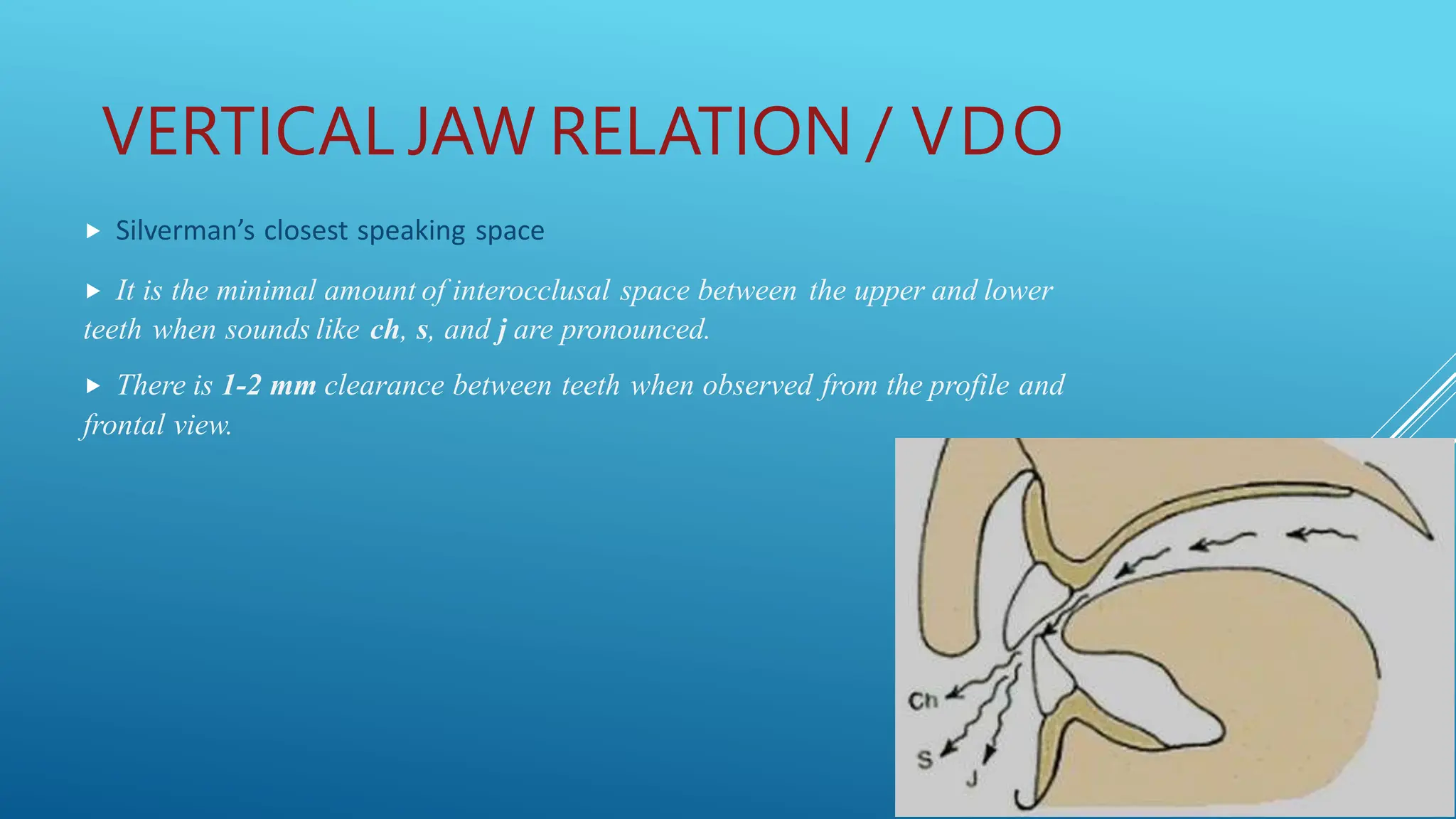
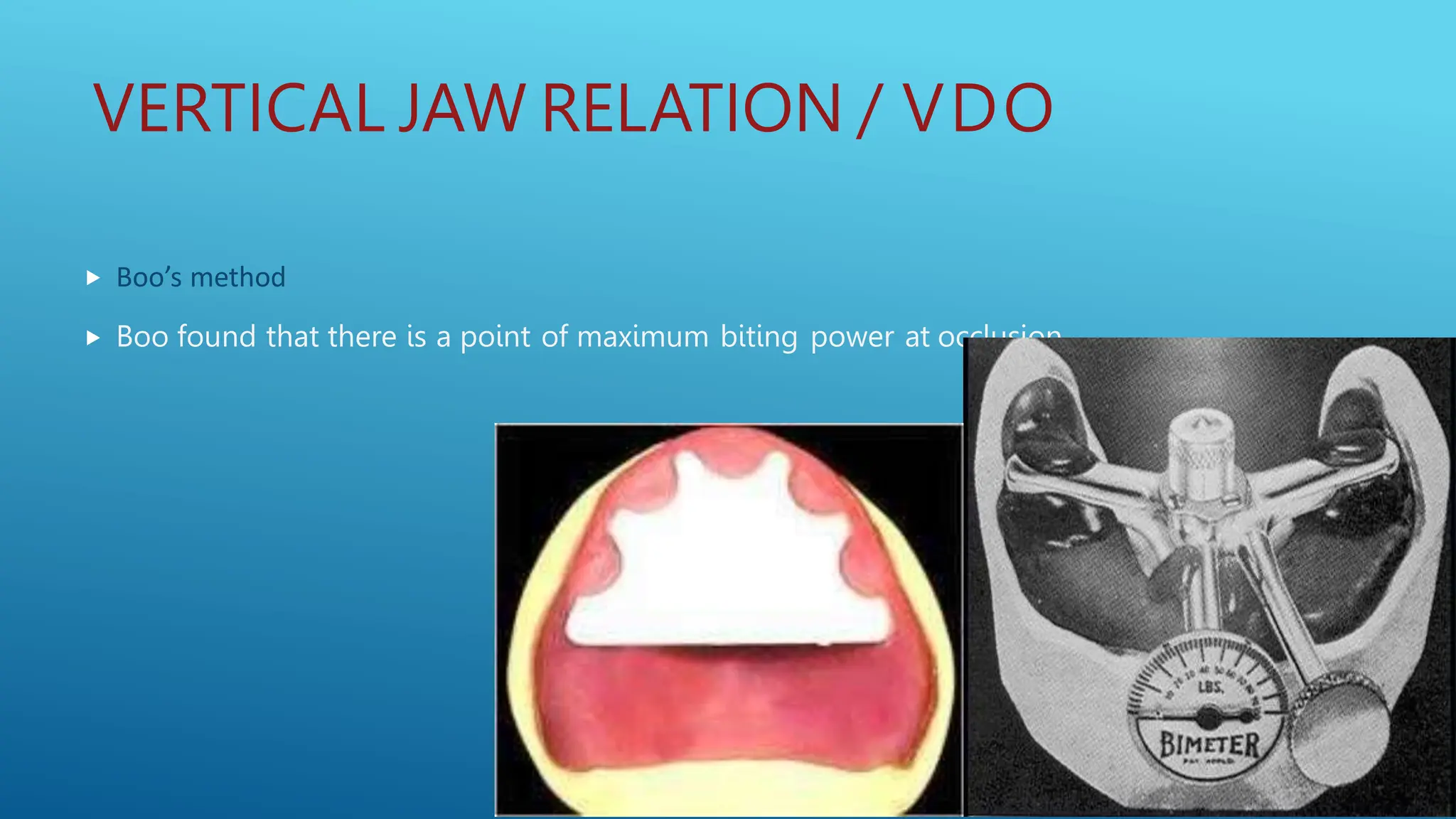
This document discusses jaw relations for complete and partial dentures. For complete dentures, it describes orientation, vertical, and horizontal relations. Orientation involves the positioning of the mandible. Vertical relation involves determining the vertical dimension of occlusion. Methods described include Niswonger's method and tactile sense. Horizontal relation involves centric and eccentric jaw positions. Centric relation is recorded using methods like needle articulation. Eccentric relations include protrusive and lateral movements. For partial dentures, methods for establishing occlusal relationships are described, including direct apposition of casts and using occlusion rims.












































































![vertical jaw relation [Autosaved].pptx .](https://cdn.slidesharecdn.com/ss_thumbnails/verticaljawrelationautosaved-250920192706-cb5ca831-thumbnail.jpg?width=640&height=640&fit=bounds)






















