Downloaded 2,276 times











![• PROGNOSTIK [Dentsply]
It detects the presence of serine proteinase and elastase in
GCF samples.
• PERIOGARD [Colgate]
It detects the presence of Aspartate Aminotransferase in GCF
sample.
• EVALUSITE
This chair side immunoassay detects periodontal pathogens
such as Aa commitans , P gingivalis , P intermedia .
91](https://image.slidesharecdn.com/seminar8-150408111915-conversion-gate01/85/chronic-periodontitis-91-320.jpg)
![• BIOLISE
Recently a software has been made Biolise [SLT-Lab instruments, Craitsheim,
Germany] which is used to detect the elastase activity in GCF.
[Hermann et al 2001].
• GLUCOMETER
It is used for Blood glucose measurements using gingival crevicular blood.
94](https://image.slidesharecdn.com/seminar8-150408111915-conversion-gate01/85/chronic-periodontitis-94-320.jpg)





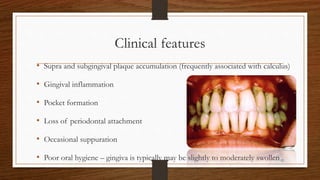
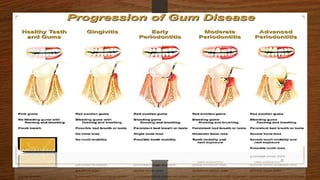
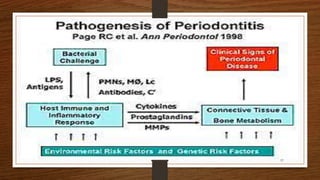
Chronic periodontitis is an inflammatory disease that causes the destruction of the tissues that support the teeth. It is caused by bacterial plaque accumulating at and below the gumline. The disease is characterized by pocket formation, attachment loss, and bone loss. It is usually slowly progressive and can range from mild to severe. Diagnosis involves measuring pocket depths, attachment levels, bleeding, and bone loss visible on radiographs. Risk factors include poor oral hygiene, smoking, diabetes, and genetic factors. Treatment aims to eliminate plaque and bacteria through nonsurgical methods like scaling and root planing or sometimes surgical procedures to reduce pocket depths and regenerate lost tissues.































































































