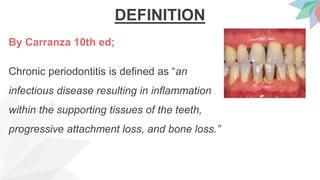
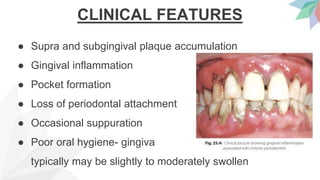
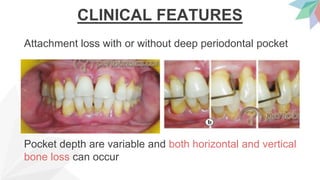
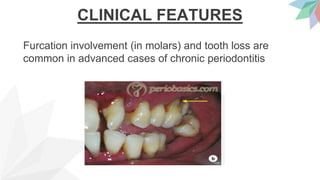
Chronic periodontitis is the most common form of periodontitis. It is characterized as a slow progressing, chronic inflammatory disease caused by bacterial plaque that leads to progressive loss of attachment and bone. If left untreated, chronic periodontitis can cause deep pockets, furcation involvement, tooth mobility, and eventual tooth loss. Risk factors include poor oral hygiene, pre-existing periodontitis, systemic diseases like diabetes, smoking, and genetic factors. Treatment involves nonsurgical and surgical therapies aimed at reducing the bacterial load and regenerating lost tissues through improved plaque control.