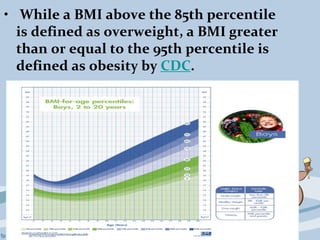
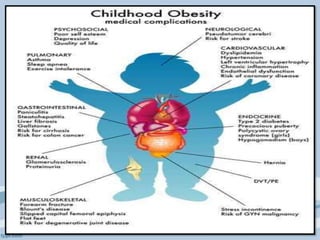
Childhood obesity is a significant health issue characterized by excess body fat affecting children's wellbeing, with a notable increase in prevalence globally. Factors contributing to obesity include genetic influences, dietary habits, and lifestyle choices, and it is diagnosed primarily using Body Mass Index (BMI) measurements. Effective prevention and management strategies involve community-based programs, multidisciplinary approaches, and, when necessary, pharmacological interventions to support healthier lifestyles in children.
![Diagnosis of childhood
obesity
• Body mass index (BMI) is acceptable for
determining obesity for children two
years of age and older.
Formula: weight (kg) / [height (m)]2
• The normal range for BMI in children
vary with age and gender.](https://image.slidesharecdn.com/childhoodobesitycollectedppt-160123163004/85/Childhood-obesity-collected-ppt-5-320.jpg)