Downloaded 51 times
![Dominick M. Maino, O.D., M.Ed., F.A.A.O ., F.C.O.V.D-A. Professor, Pediatrics/Binocular Vision Service Illinois College of Optometry Illinois Eye Institute 3241 S. Michigan Ave. Chicago, Il. 60616 312-949-7280 (Voice) 312-949-7358 (fax) [email_address] MainosMemos.blogspot.com www.ico.edu nw.optometry.net](https://image.slidesharecdn.com/childspecialneeds1-110912180245-phpapp01/85/Child-with-Special-Needs-Part-1-2-320.jpg)

![Questions? Contact: Dominick M. Maino, OD, MEd, FAAO,FCOVD-A Professor, Pediatric/Binocular Vision Service Illinois Eye Institute Illinois College of Optometry 3241 S. Michigan Ave. Chicago, Il. 60616 312-949-7280 (phone) 312-949-7660 (fax) [email_address] www.ico.edu www.nw.optometry.net MainosMemos.blogspot.com](https://image.slidesharecdn.com/childspecialneeds1-110912180245-phpapp01/85/Child-with-Special-Needs-Part-1-89-320.jpg)

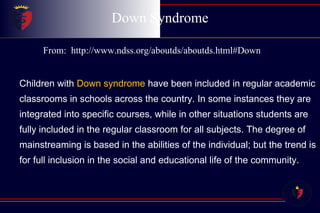
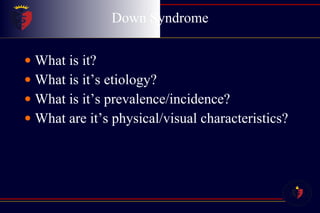
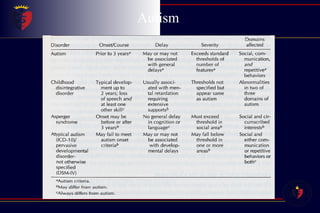
This document provides information on Down syndrome including: - Down syndrome is a genetic condition caused by trisomy 21 and has a prevalence of 1 in 800-1000 live births. - Physical characteristics include refractive errors like hyperopia and astigmatism as well as binocular vision issues like strabismus. - Recent studies have found that bifocals can effectively treat the reduced accommodation often seen in individuals with Down syndrome.





















































![Child special needs 1 [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/childspecialneeds1compatibilitymode-110912174329-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)


















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

