Downloaded 11 times
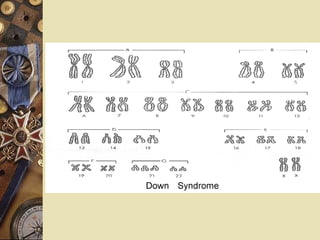
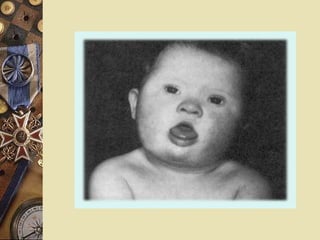
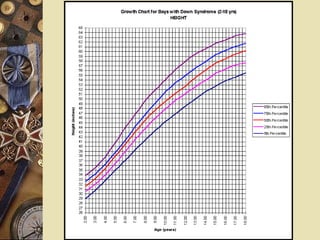


Down syndrome is a genetic disorder caused by trisomy 21, occurring in approximately 1 in 1000 live births. It is characterized by intellectual disability and distinctive facial features such as a flat nasal bridge and upward slanting eyes. Individuals with Down syndrome often experience certain health problems as well, including heart defects, gastrointestinal abnormalities, hearing or vision issues. Proper management includes ongoing screening and treatment to address common medical comorbidities. With improved healthcare, the average life expectancy for individuals with Down syndrome has risen significantly in recent decades.






























![[송년특강] 페이스북 타임라인 활용가이드 111229](https://cdn.slidesharecdn.com/ss_thumbnails/111229-111229190825-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)























































