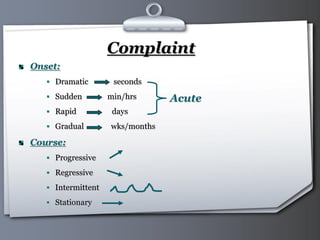
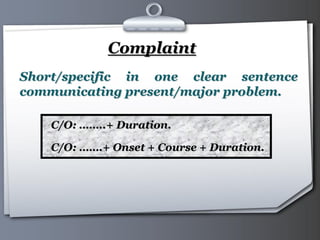
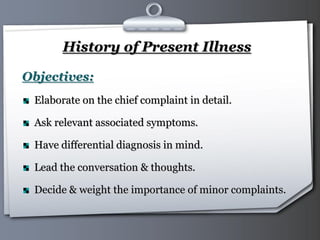
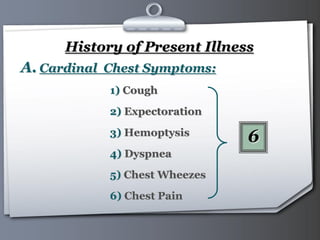
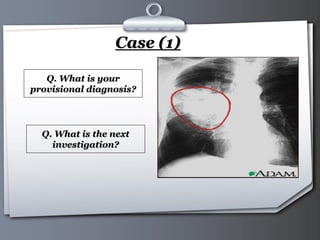
This document provides guidance on taking a chest history from patients. It discusses the importance of history taking in making an accurate diagnosis. The general approach to history taking is described, including introducing oneself, treating the patient with respect, listening, and asking clear questions. Specific aspects of the chest history are then covered in detail, including personal history, chief complaint, history of present illness, past history, and family history. Cardinal and minor chest symptoms are defined. Case examples are presented to demonstrate applying the history to form a provisional diagnosis and plan appropriate investigations.