1. Dyspnea, or breathlessness, is a common and debilitating symptom that affects many patients presenting to hospitals and clinics.
2. Dyspnea can have cardiac or pulmonary causes, and a thorough assessment is needed to determine the underlying reason for the symptom. Key parts of the assessment include evaluating dyspnea based on exertion level, as well as signs like orthopnea and paroxysmal nocturnal dyspnea.
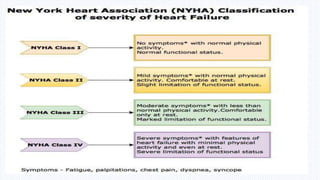
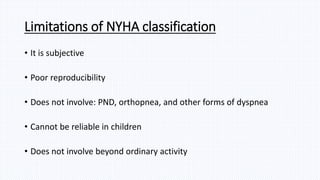
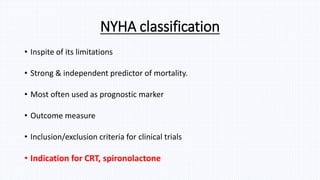
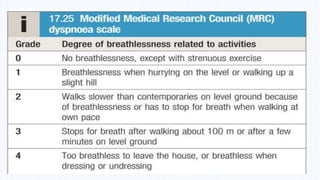
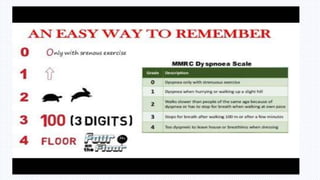
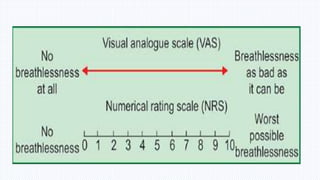
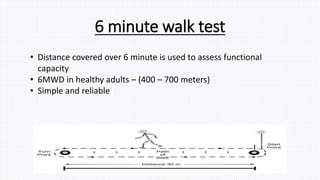
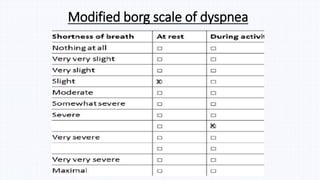
3. Grading scales like NYHA and mMRC can help classify the severity of dyspnea and predict outcomes. Features like duration of symptoms and time between dyspnea and edema onset also provide useful clinical information.




































![[Int. med] dyspnoea](https://cdn.slidesharecdn.com/ss_thumbnails/int-150502144320-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)















































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)




![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)