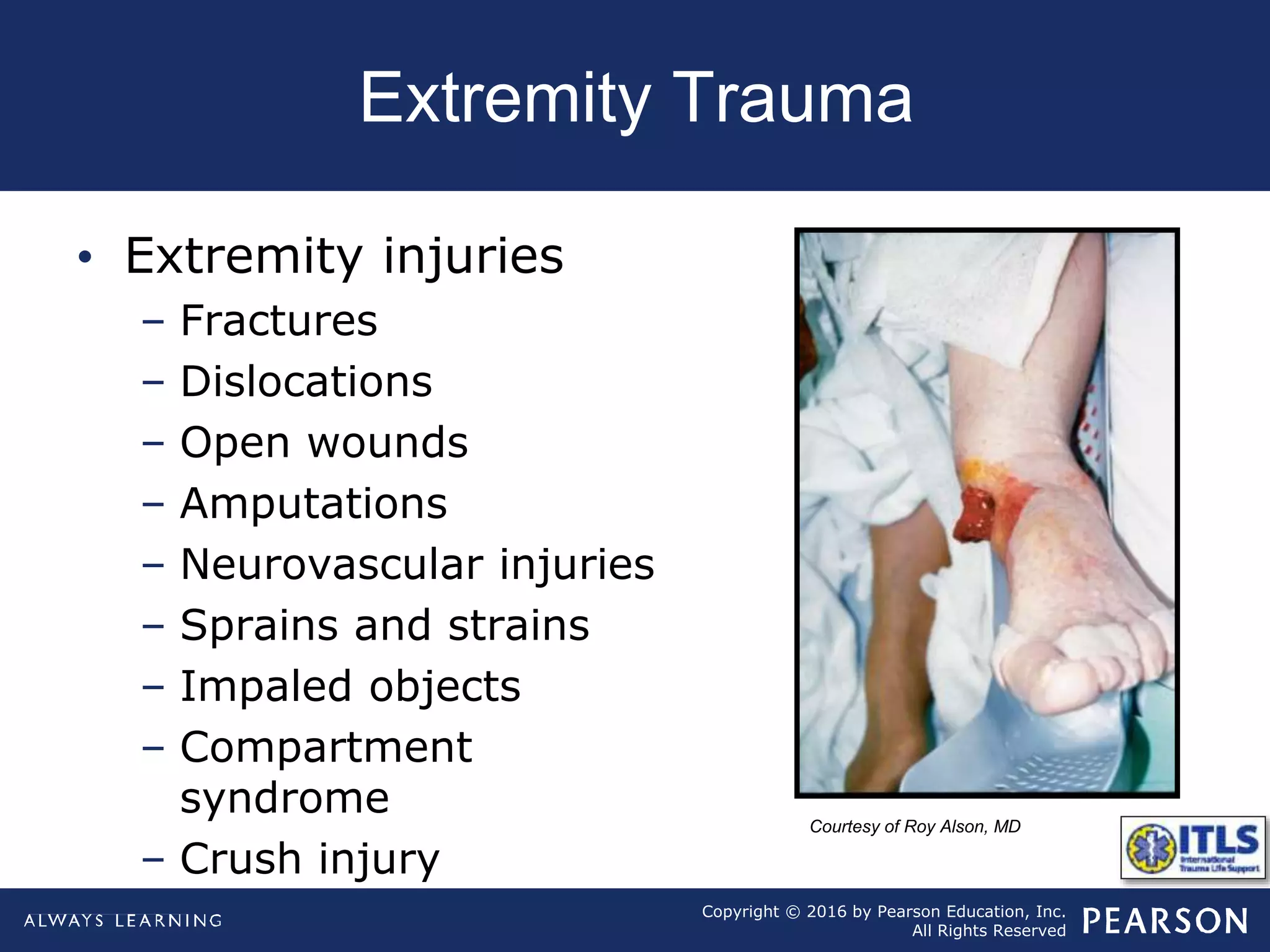
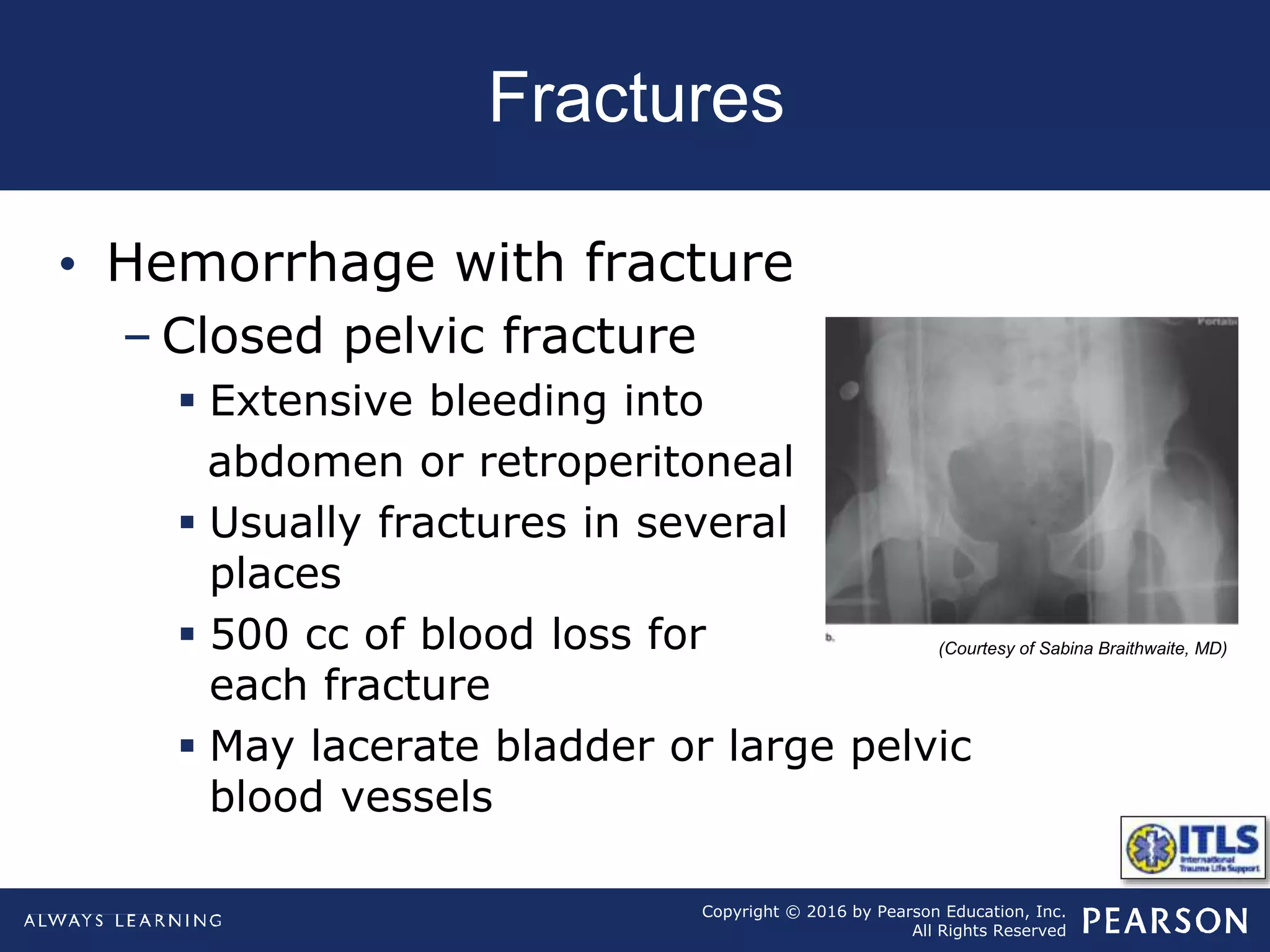
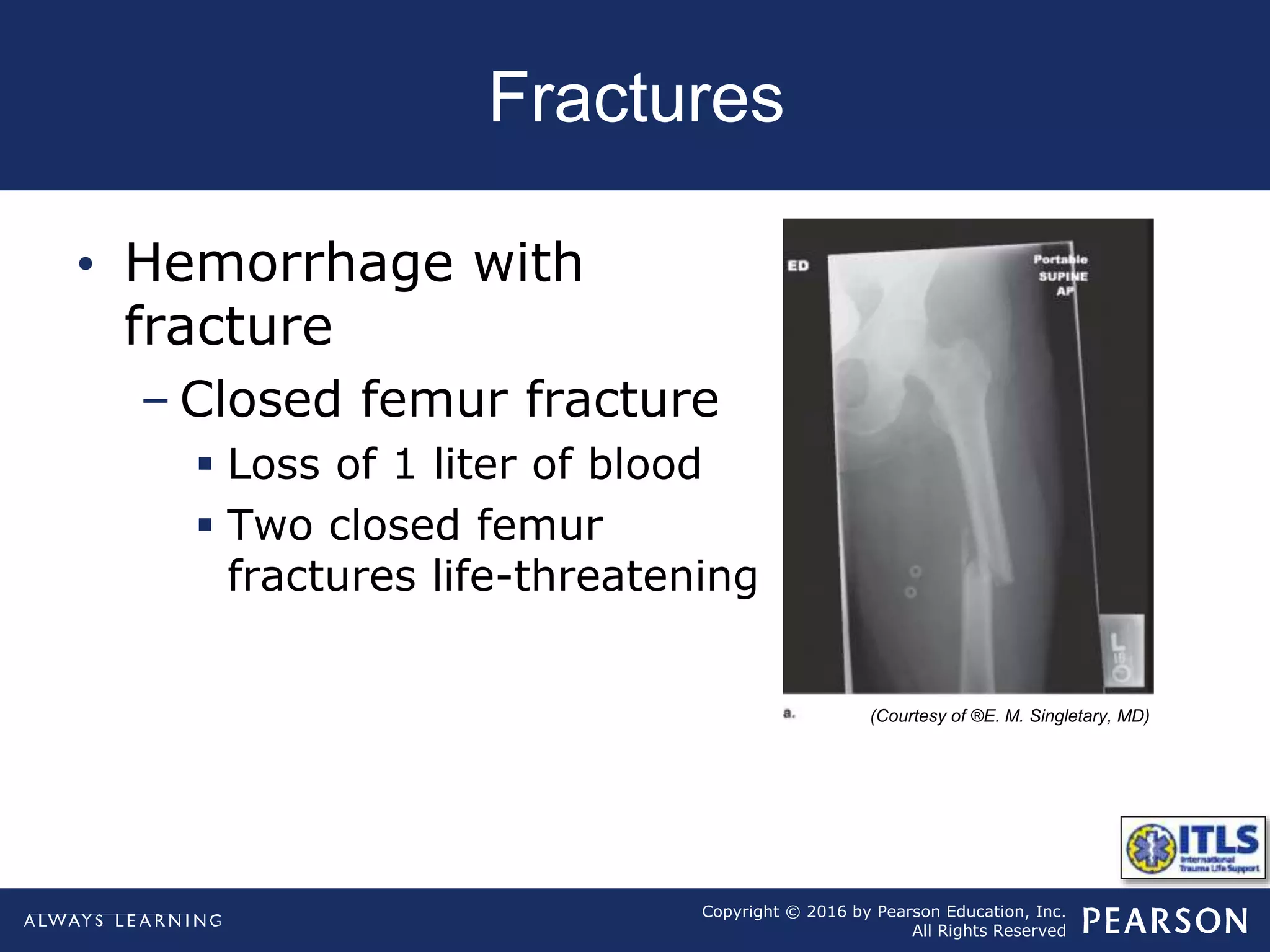
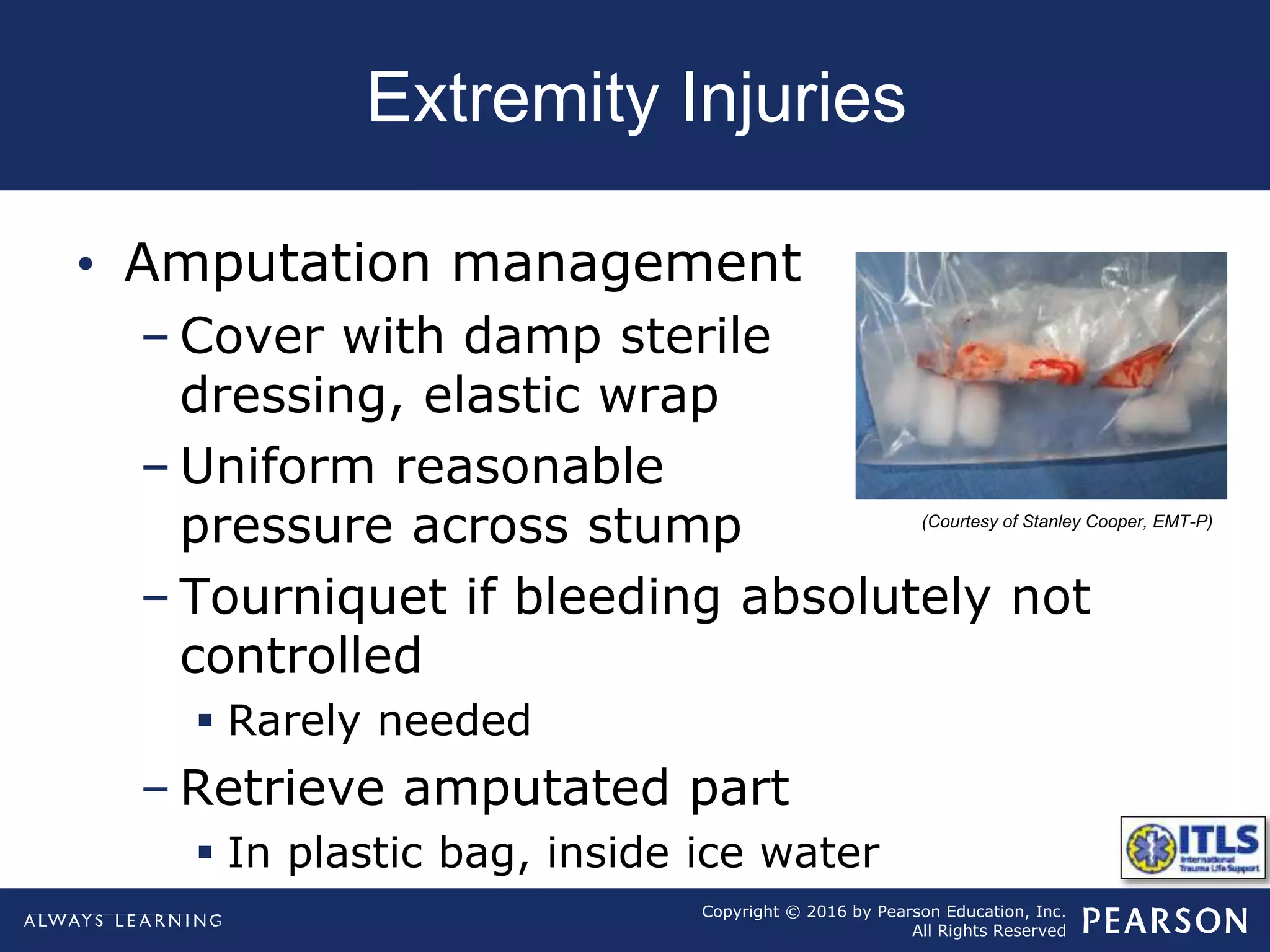
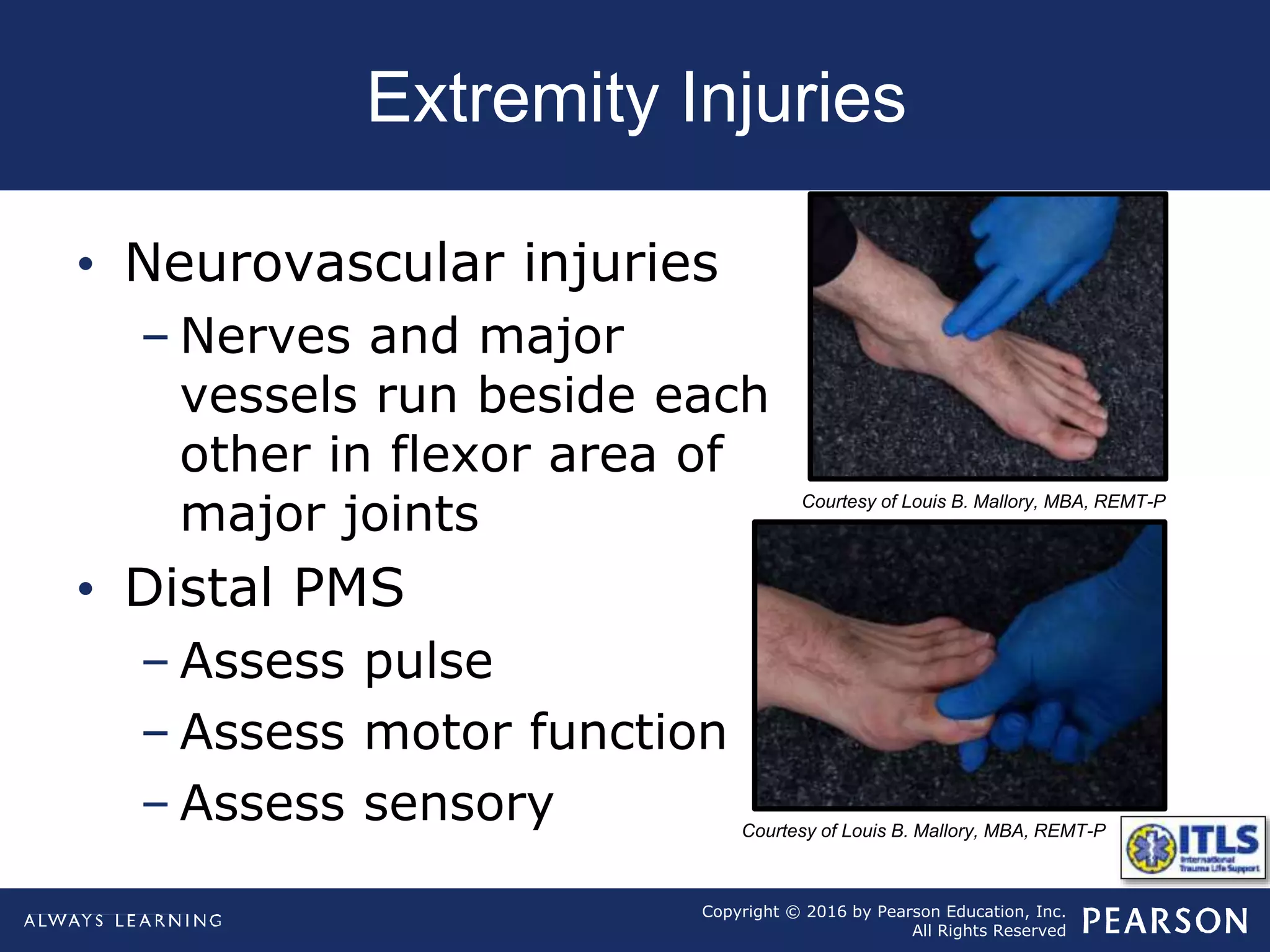
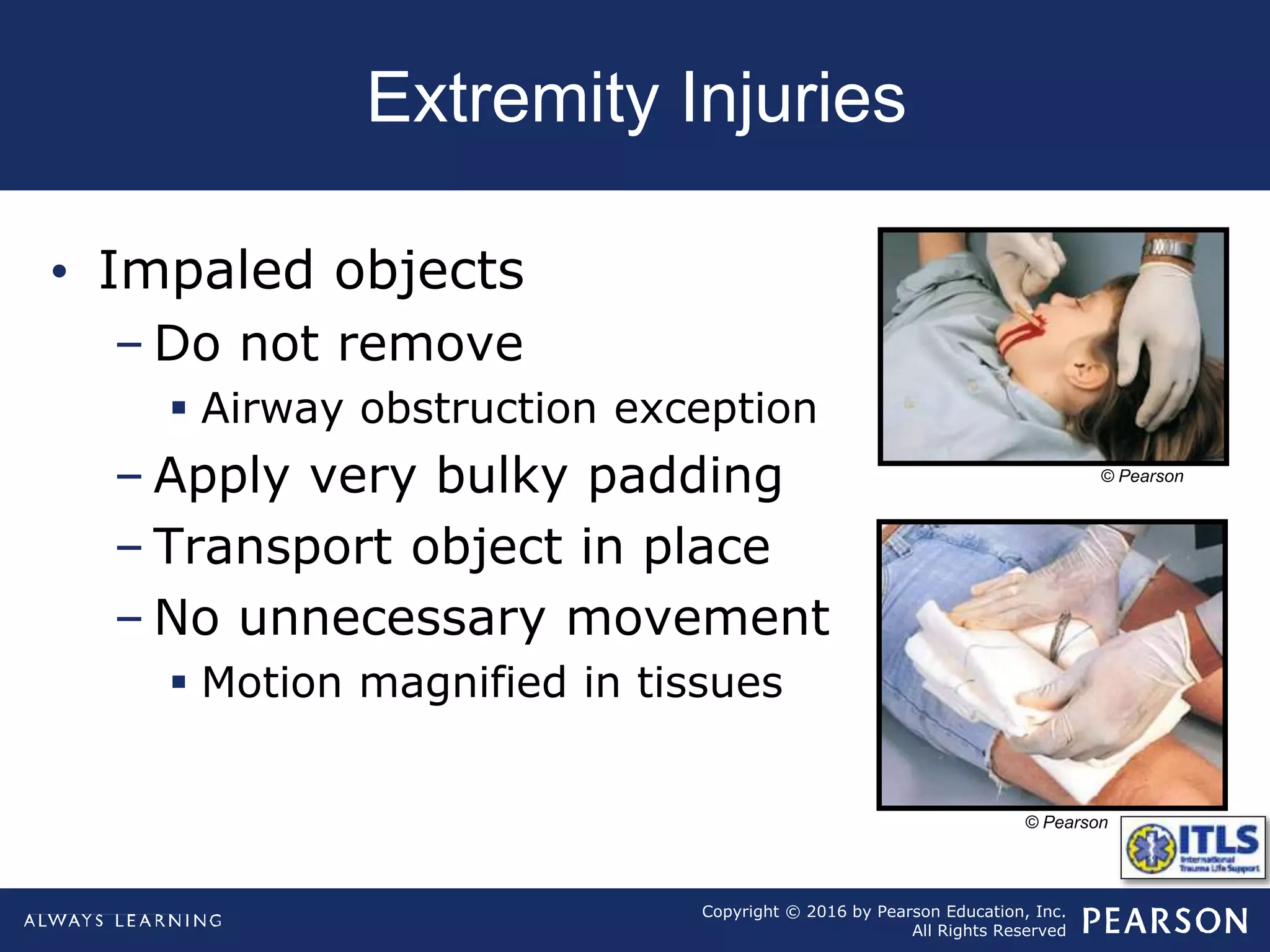
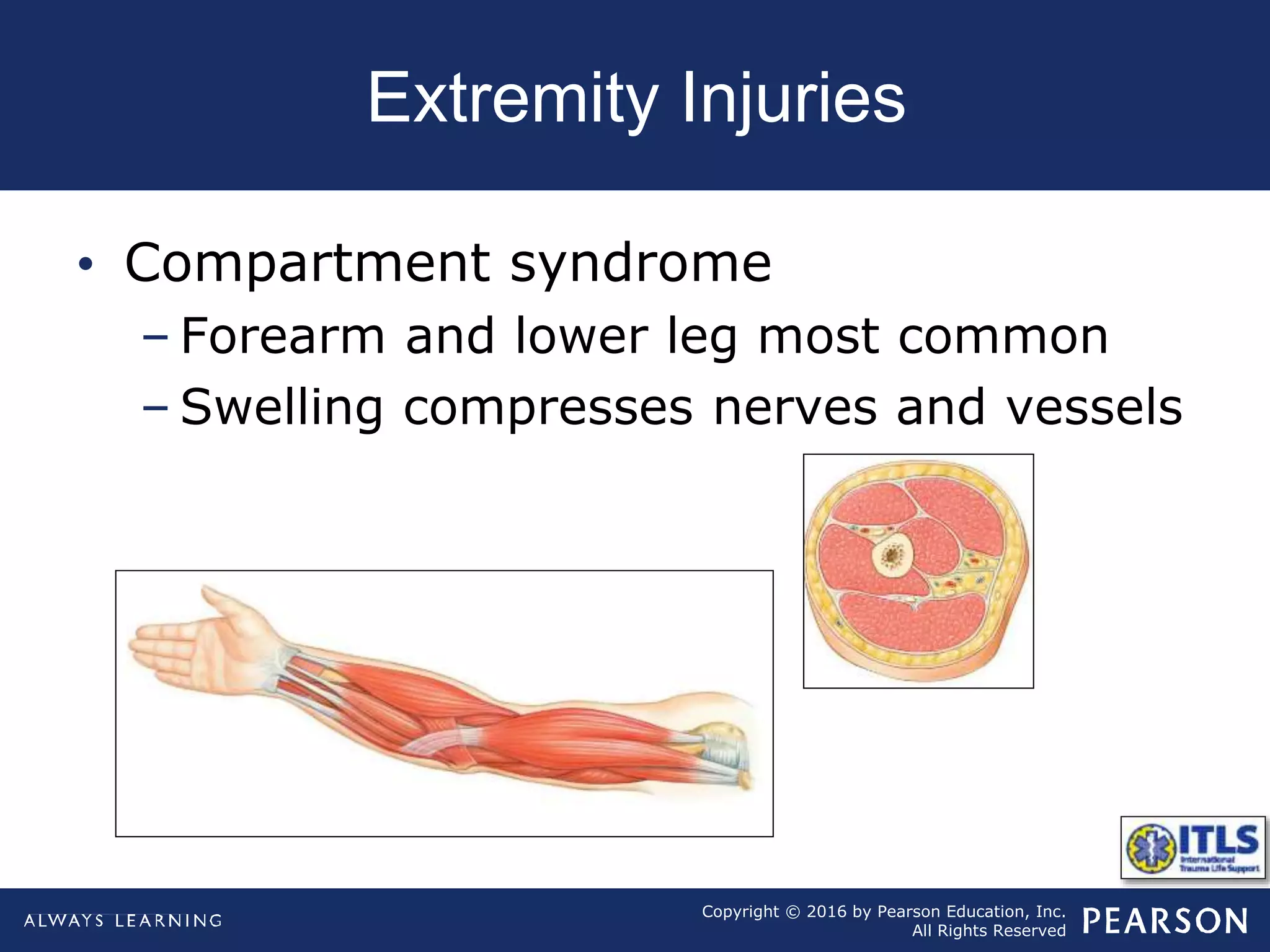
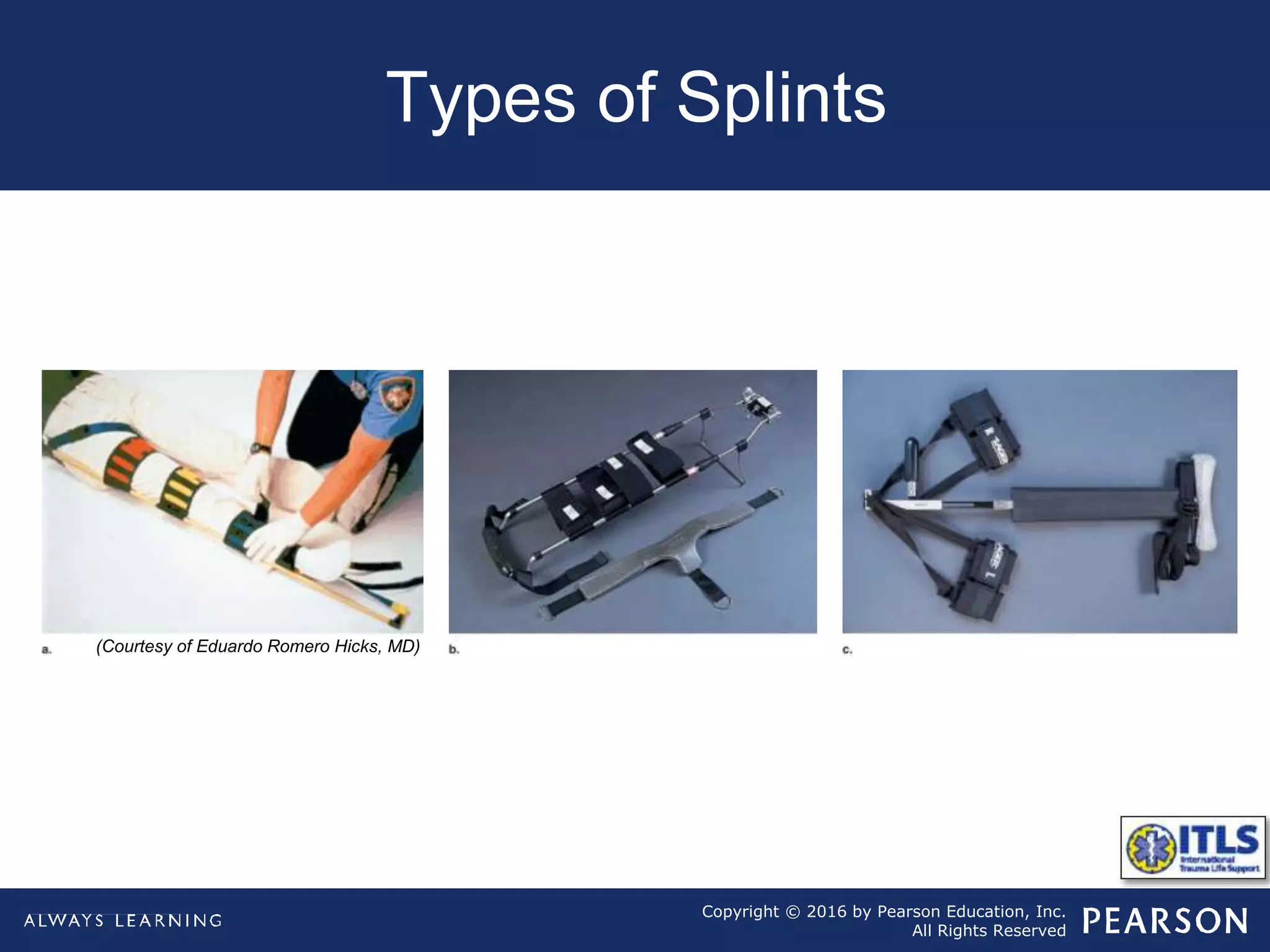
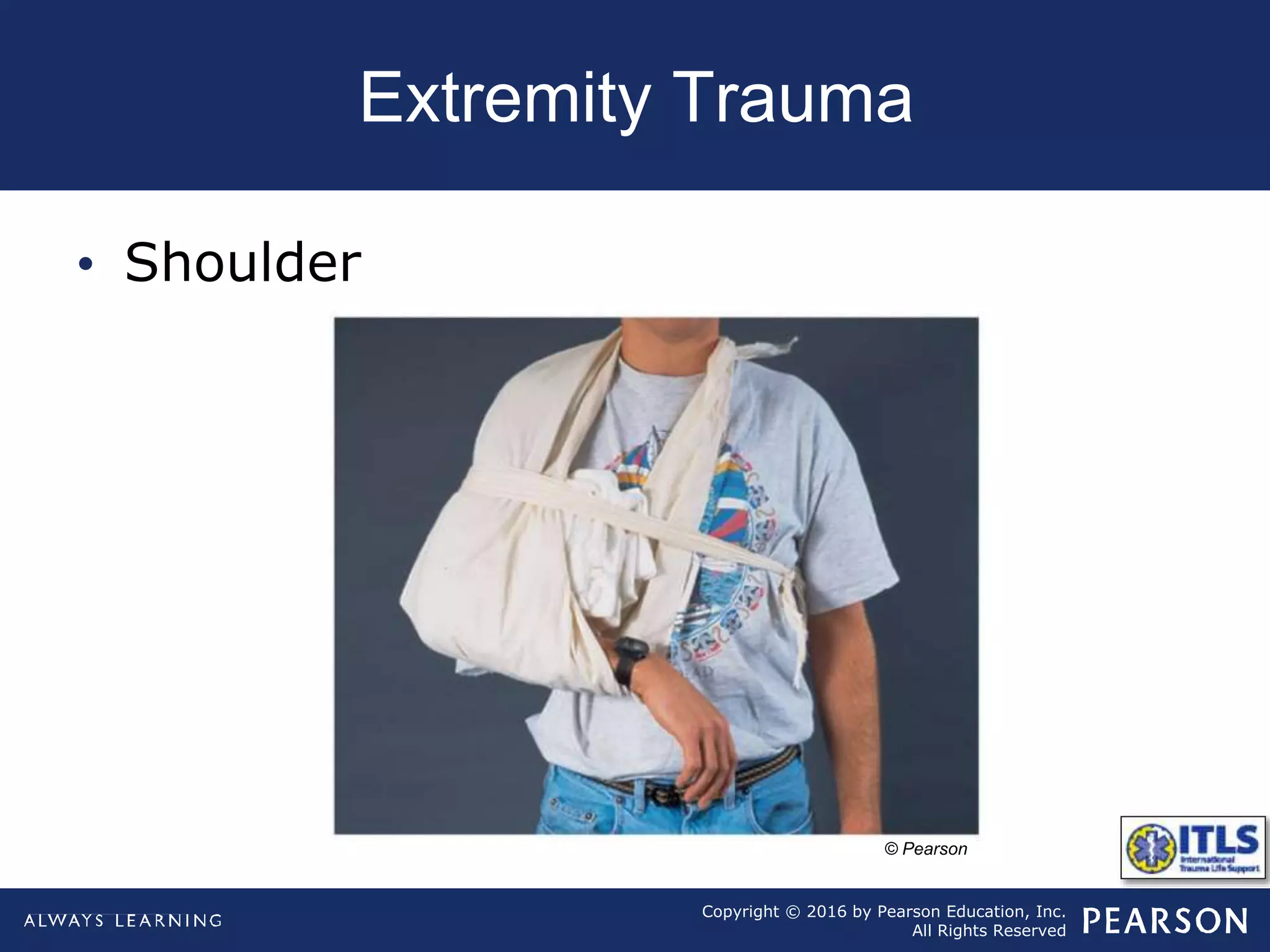
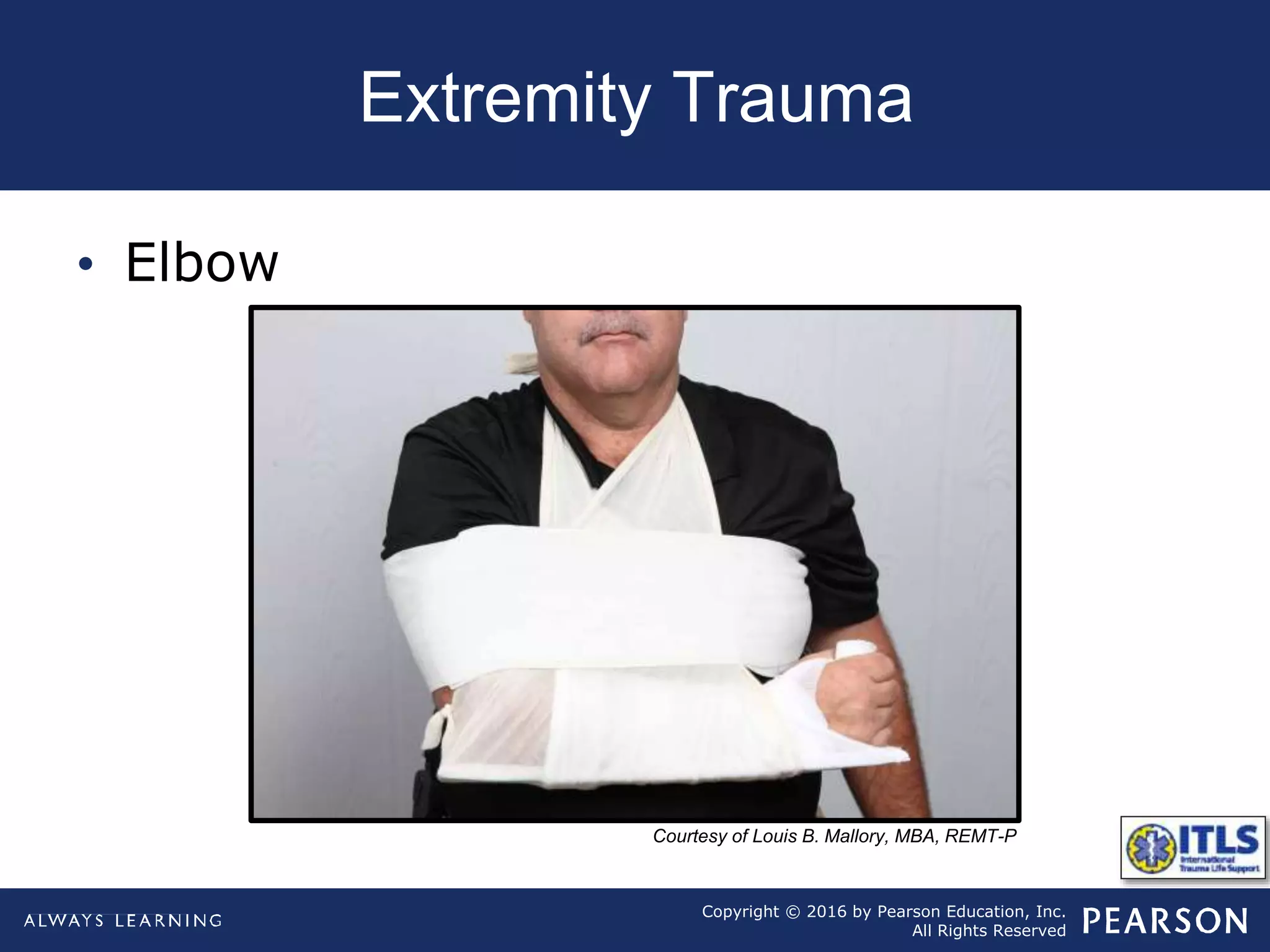
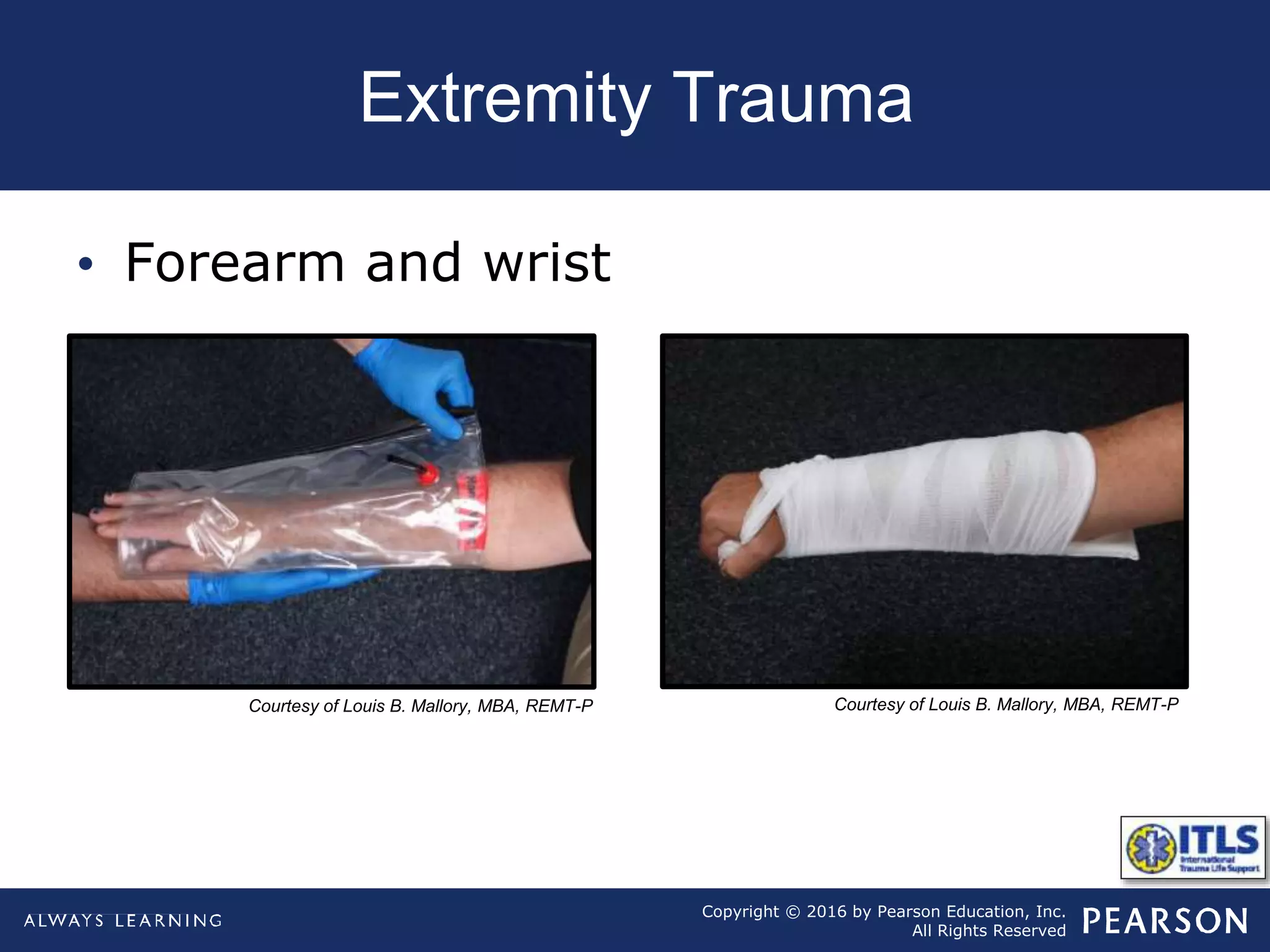
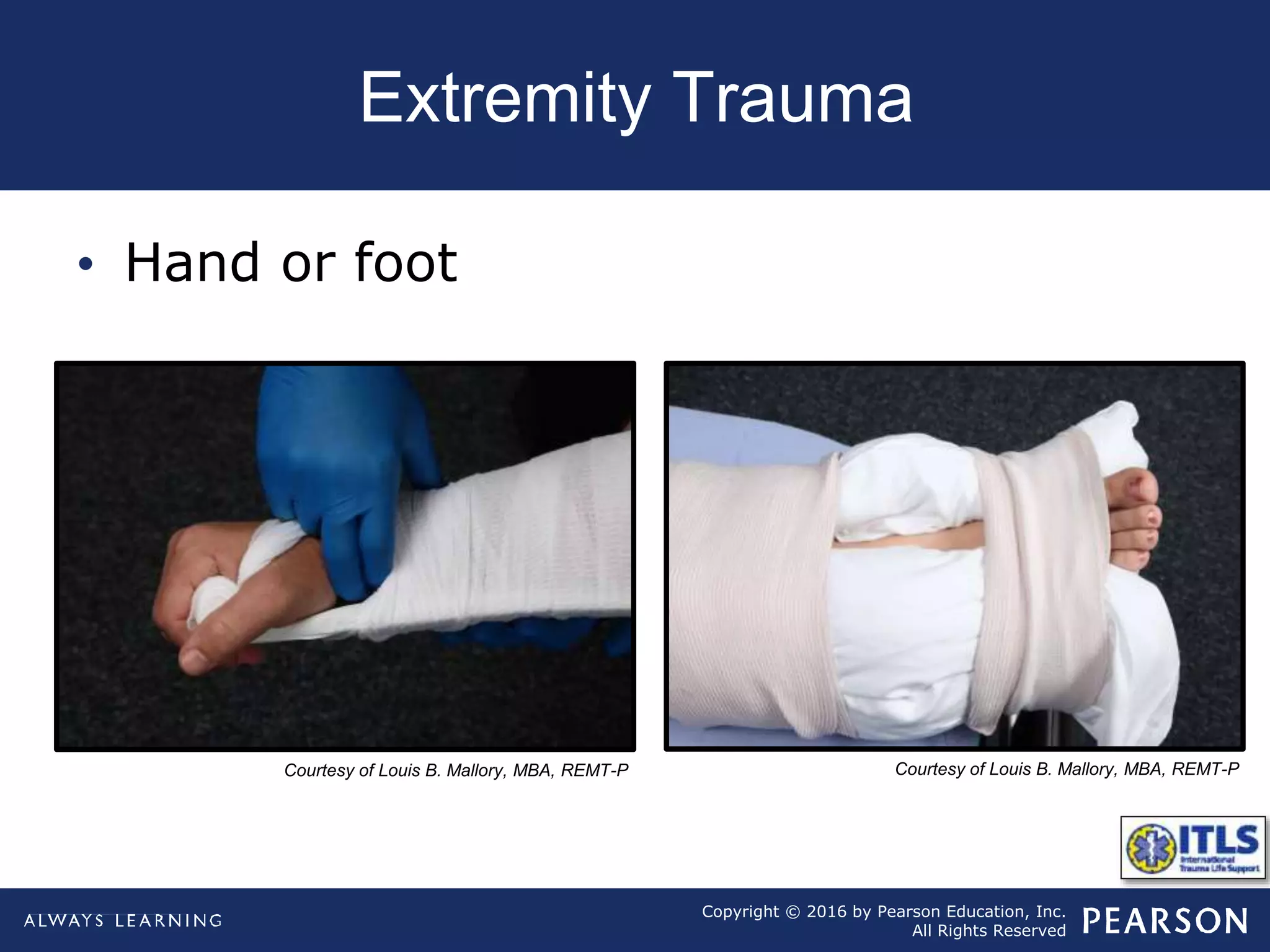
The document discusses extremity trauma, including fractures, dislocations, open wounds, amputations, and other injuries. It emphasizes that extremity injuries are generally not life-threatening, but can cause disability or complications like hemorrhage or compartment syndrome. The key priorities are to address any life-threatening injuries first, check neurovascular status, control bleeding, clean and dress wounds, splint suspected fractures to prevent further injury, and watch for signs of compartment syndrome.