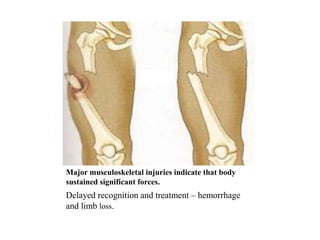
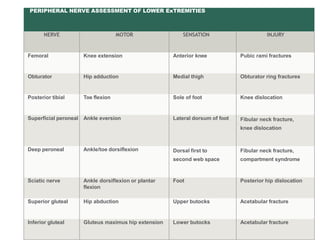
This document summarizes key points about musculoskeletal trauma presented by Dr. Mohit Garg. It discusses resuscitation of patients with extremity injuries, including controlling hemorrhage from injuries like arterial bleeding, traumatic amputations, bilateral femoral fractures, and crush syndrome. It also covers assessment and management of open fractures, vascular injuries, compartment syndrome, and neurological injuries. Physical examination involves identifying life-threatening and limb-threatening injuries by looking for deformities, feeling for areas of tenderness, and evaluating circulation and sensation. X-rays may be needed but not if there is vascular compromise or risk of skin breakdown.