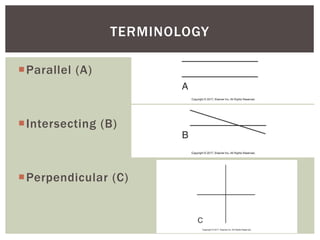
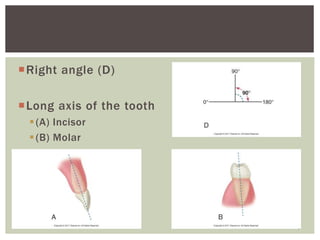
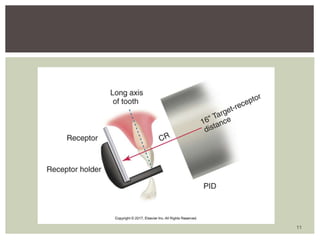
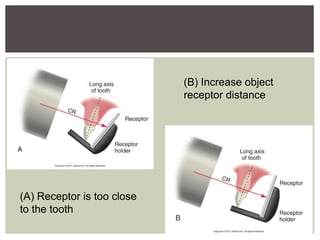
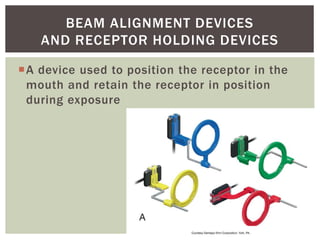
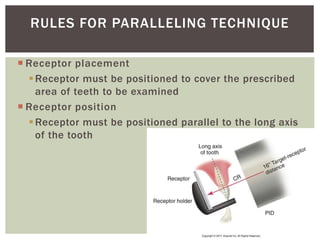
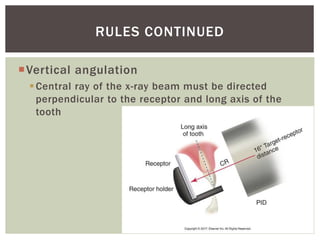
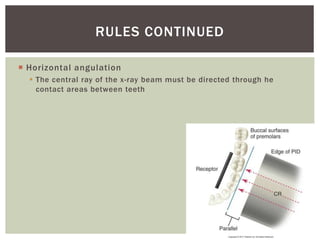
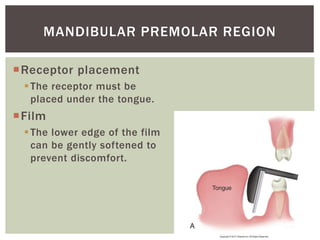
The document outlines the learning objectives and procedures for using the paralleling technique in dental radiography. It defines key terms, states the basic principle of keeping the receptor parallel to the tooth, and describes the placement of equipment. Rules for the technique include keeping the central ray perpendicular to the receptor and long axis of the tooth. Patient preparation, exposure sequencing, and modifications for anatomical variations are discussed. The primary advantage is producing images without dimensional distortion.