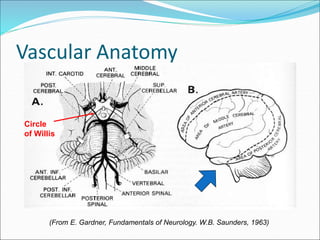
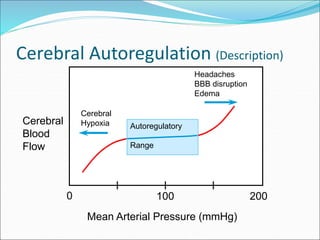
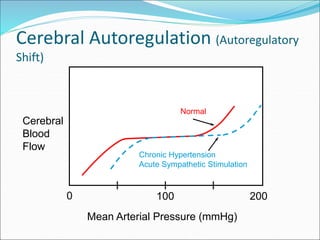
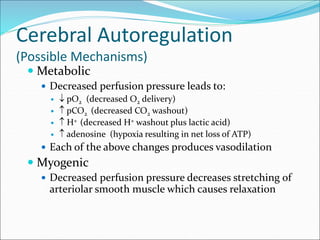
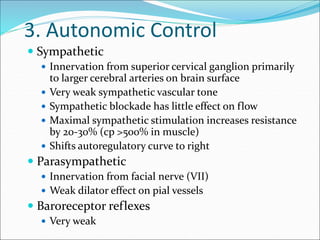
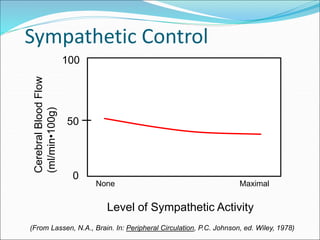
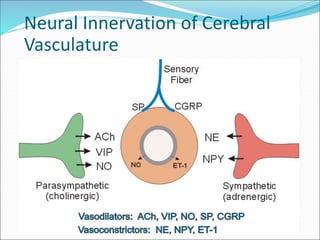
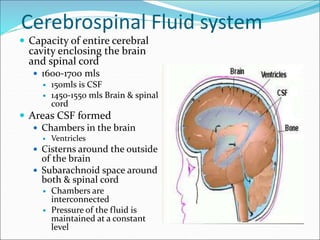
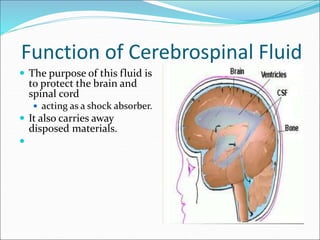
This document discusses cerebral blood flow and its regulation. It begins by outlining the clinical importance of abnormalities in blood flow, metabolism, fluids, composition, pressure and how they profoundly affect brain function. It then covers the vascular anatomy of the brain, control of cerebral blood flow, determinants of cerebral perfusion pressure, local and neurohumoral regulation of cerebral blood flow. Specific topics discussed in more detail include autoregulation of cerebral blood flow, effects of intracranial pressure, humoral control including catecholamines and neuropeptides, neural innervation, cerebrospinal fluid system, brain barriers, and circumventricular organs.