Downloaded 1,470 times









































































![REFERENCES
Books -
[1] R.A.Cawson’s essentials of Oral Pathology and Oral
Medicine . 7th Edition
[2] Burkitts Oral Pathology 5th Edition
[3] Shafer, Hine & Levy: A textbook of oral pathology.
Articles –
1. Nanotechnology : A new era in dentistry JADA 2012
2. Oral potentially malignant disorders: Precising the definition.
Otorhinolaryngology clinics –An International journal may-sept. 2009
4. Classification of OSMF. Swati Gupta, Jigar joshi , JIAOMR
5. NEW CLASSIFICATION FOR ORAL POTENTIALLY MALIGNANT DISORDERS
S. SARODE, SARODE, KARMARKAR, TUPKARI
(Ref - Oral Oncology xxx, 2011)
6. Precancerous lesions of oral cavity.
-Uday pawar, Pankaj C. Otorhinolaryngology International Journal 2009.](https://image.slidesharecdn.com/precancerouslesionsconditions-150512133912-lva1-app6892/75/Pre-cancerous-lesions-conditions-93-2048.jpg)


The document discusses oral potentially malignant disorders (OPMD). It defines OPMD as a group of disorders that may lead to oral cancer. OPMD were previously referred to as precancerous lesions and conditions but this term was abandoned in 2005. The document categorizes OPMD into 4 groups based on etiology and pathogenesis. It provides detailed information about leukoplakia, including definition, risk factors, clinical features, histopathological grading, differential diagnosis and treatment options. Leukoplakia is considered the most common OPMD and accurate diagnosis requires biopsy and histopathological examination.
This slide outlines the contents of the presentation covering various aspects of oral cancer.
Global oral cancer incidence is 500,000/year; India has 1,00,000 cases annually, 40% of all cancers.
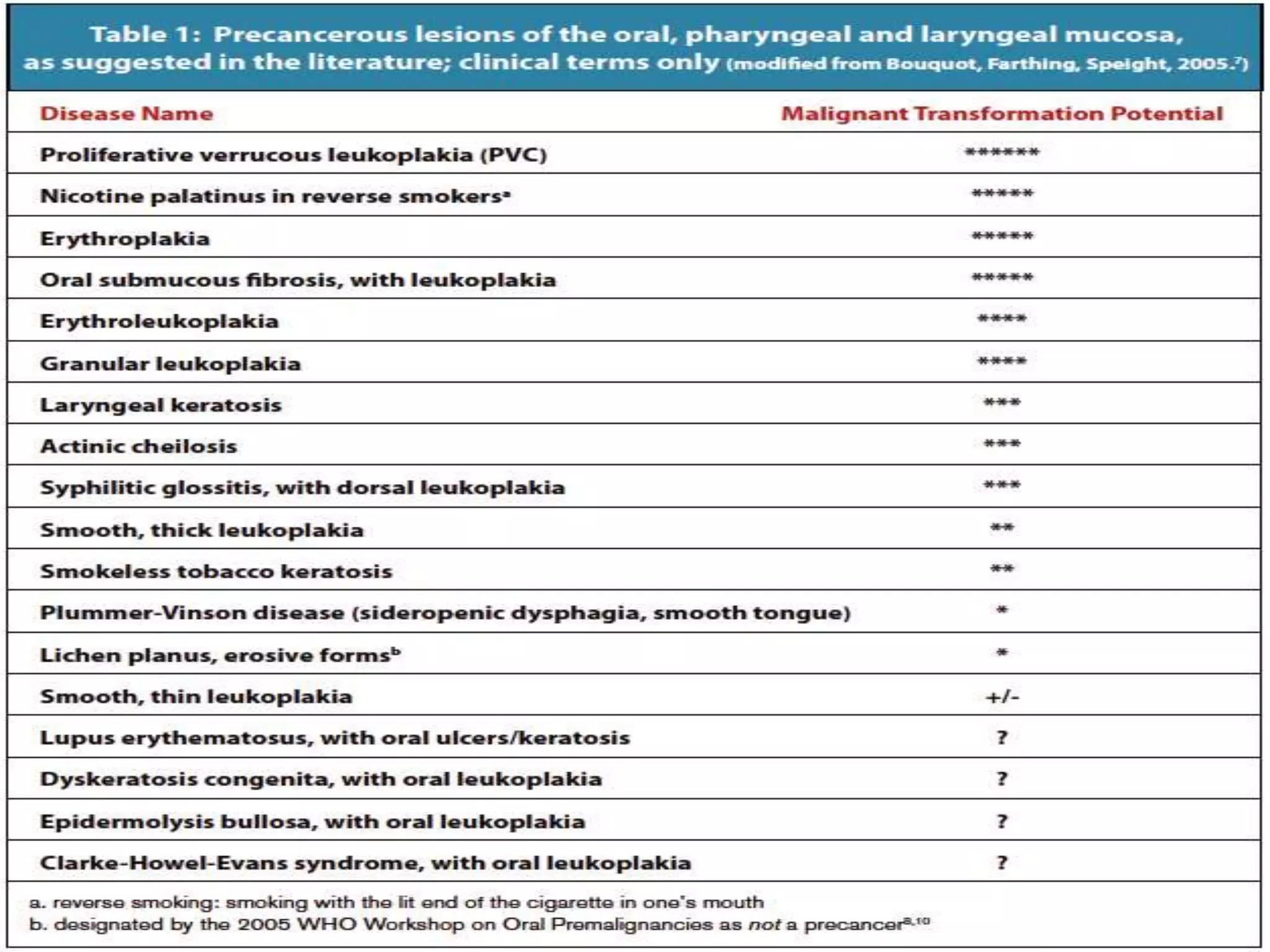
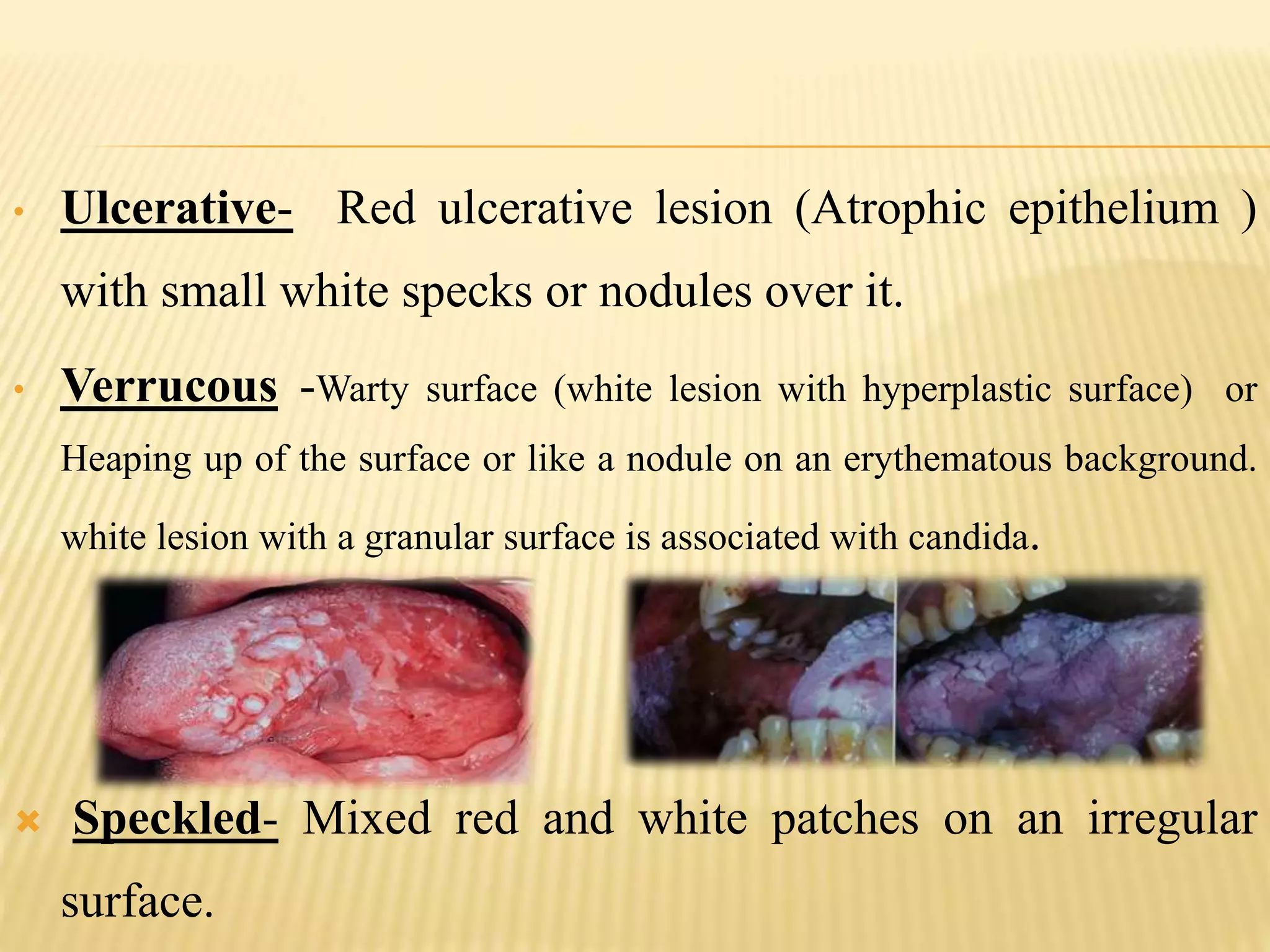
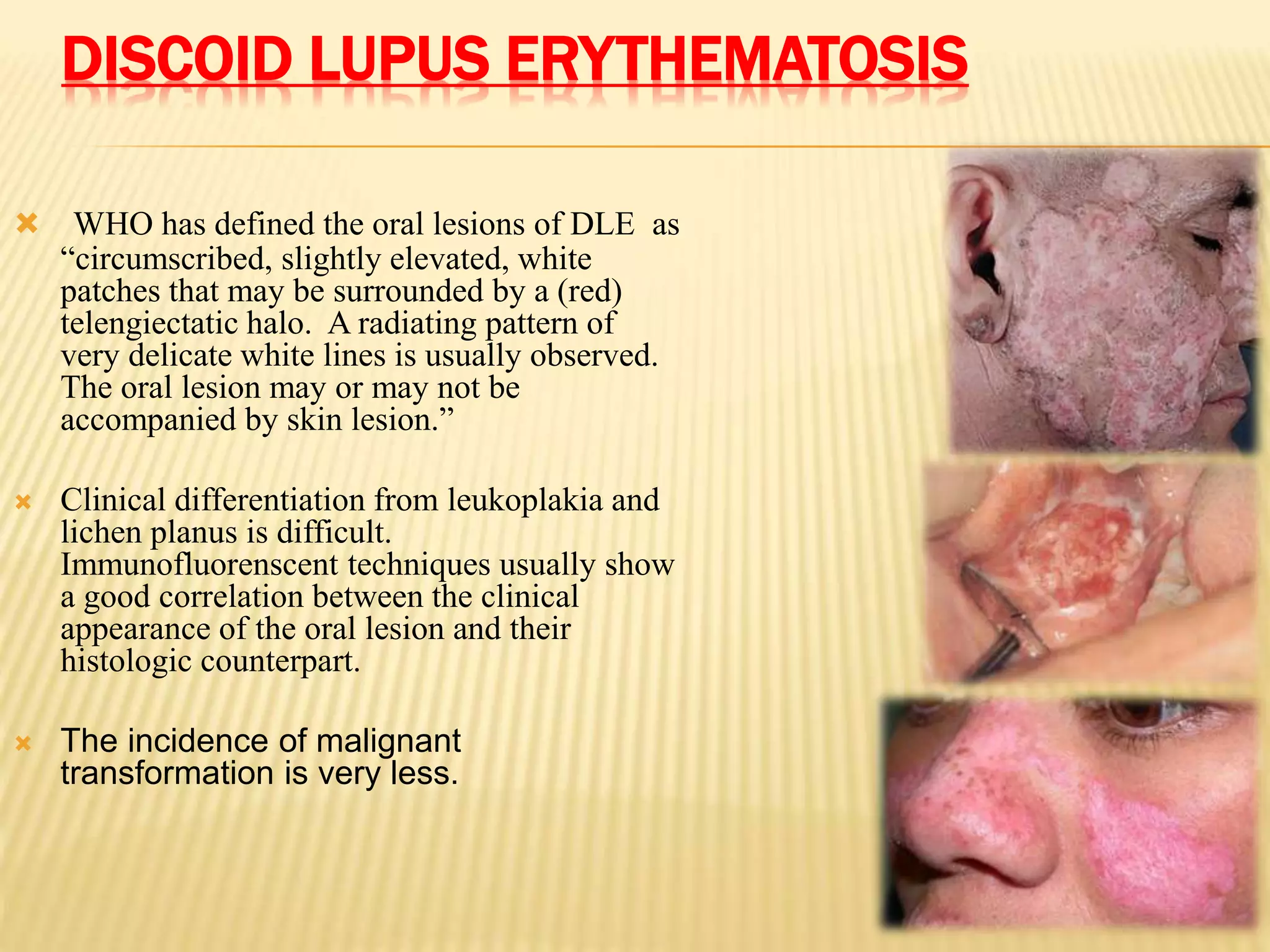
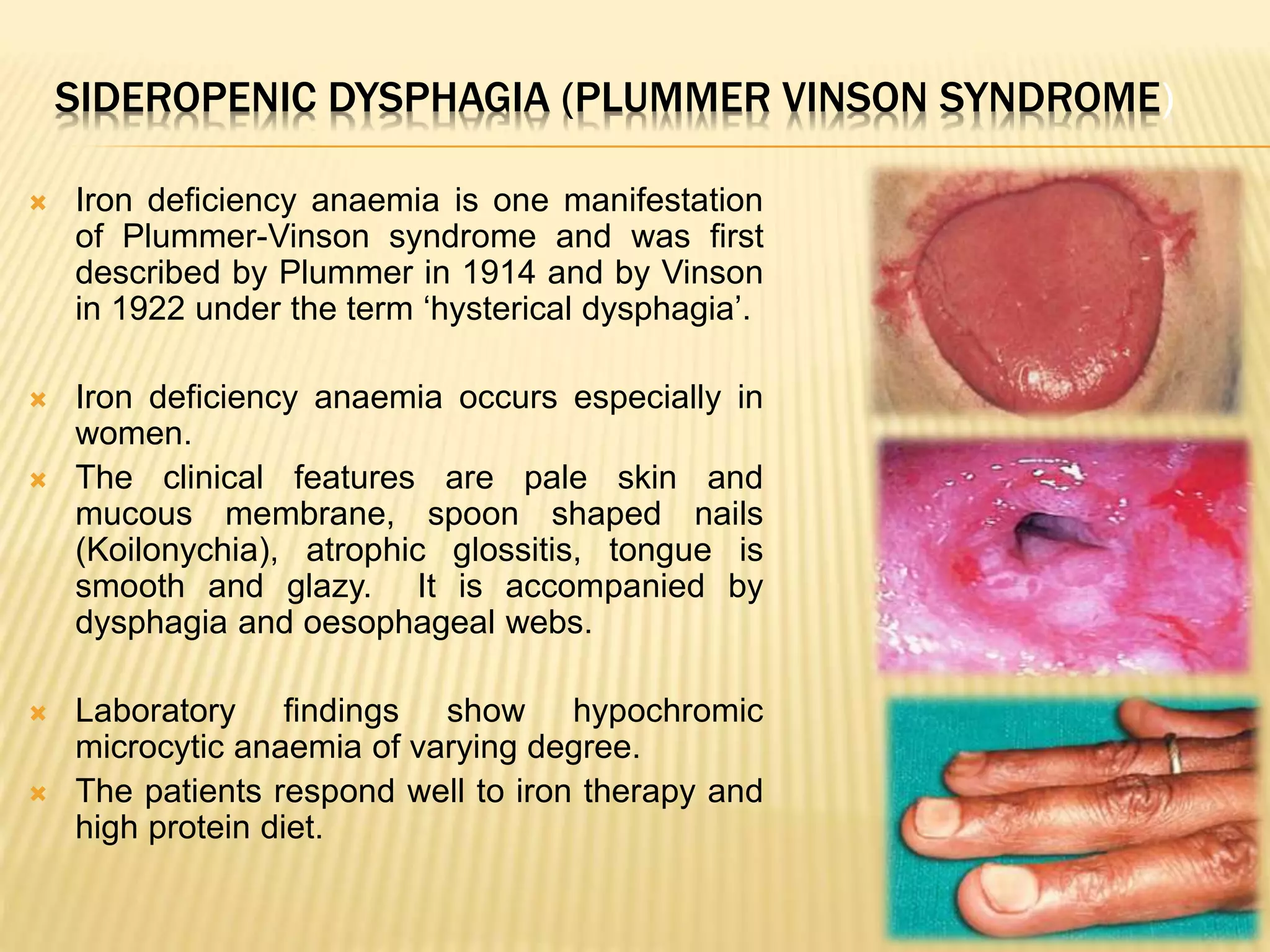
Discusses types of lesions (red/white) with potential for malignant change, and history of terminology.
Definitions of premalignant lesions/conditions and listing various associated disorders.
Definition and characteristics of PMDs with a focus on genetic and histological alterations.
Four groups of OPMD based on etiology, inflammation, inherited cancer syndromes, and susceptibility.
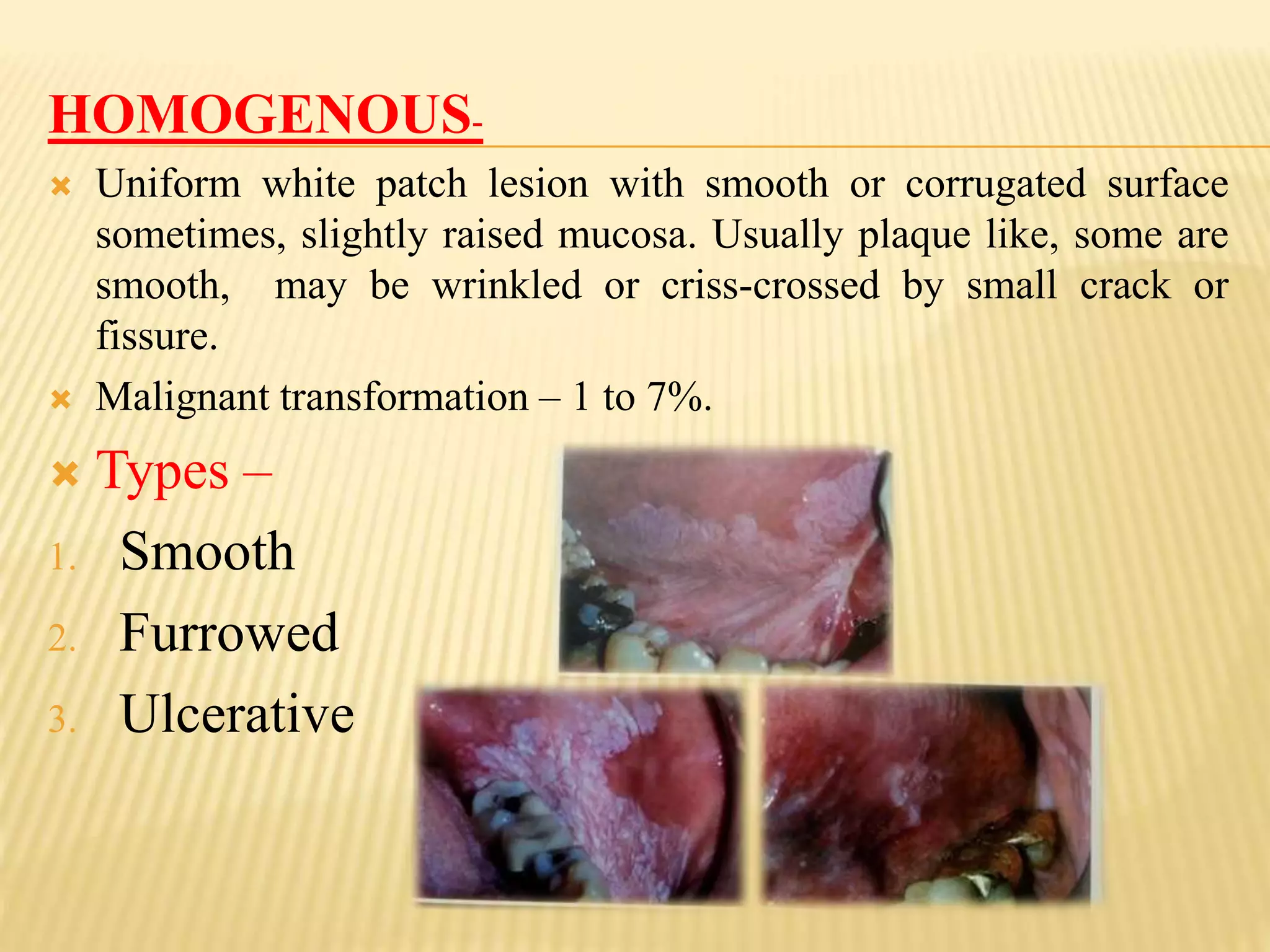
Description, etiology, and clinical features of oral leukoplakia; types and risks of malignancy.
Staging, histopathology, differential diagnosis, and treatment strategies for leukoplakia.
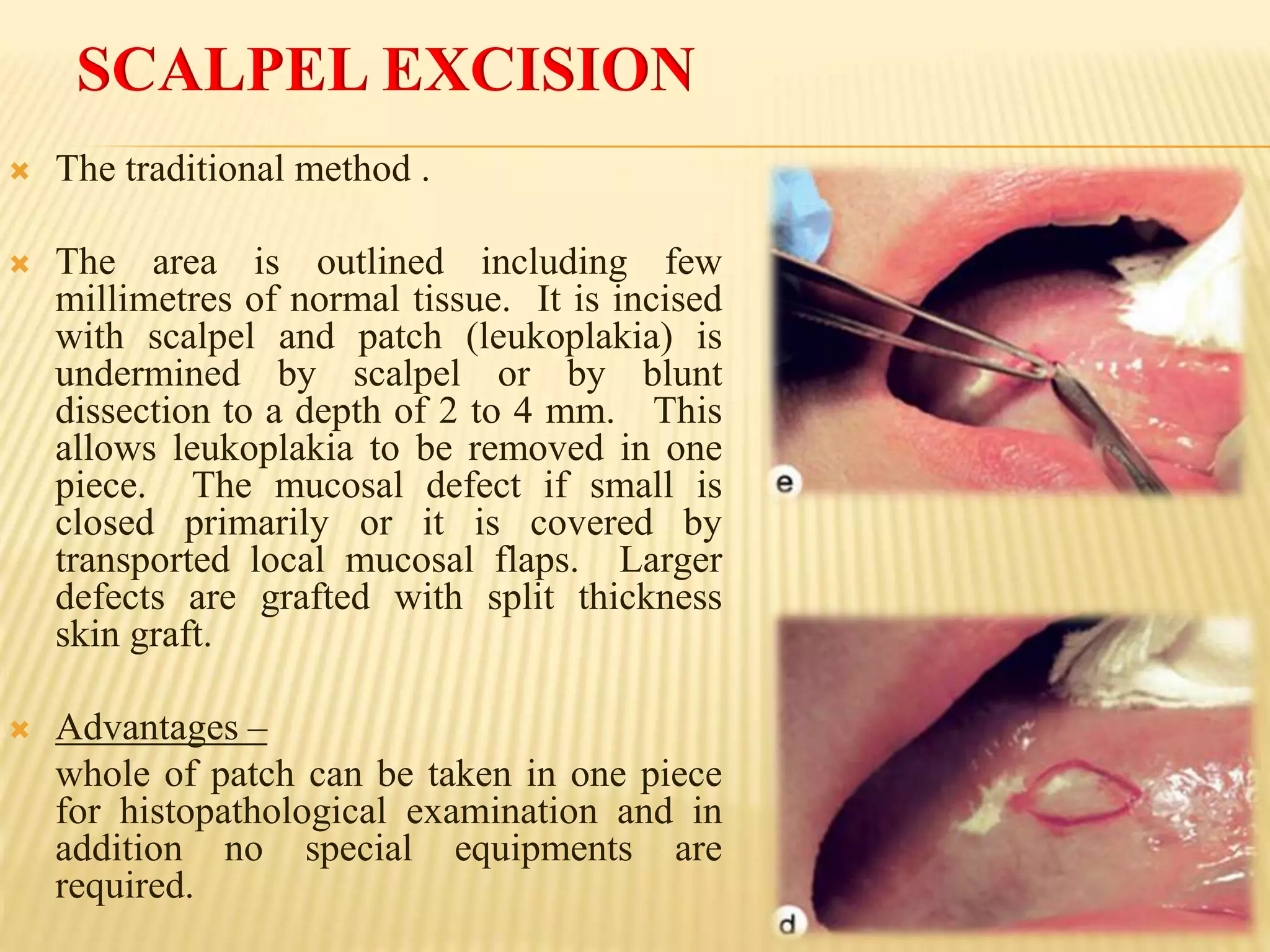
Details on chemoprevention and various surgical methods for removing leukoplakia.
Definition, clinical features, differential diagnosis, and treatment for erythroplakia.
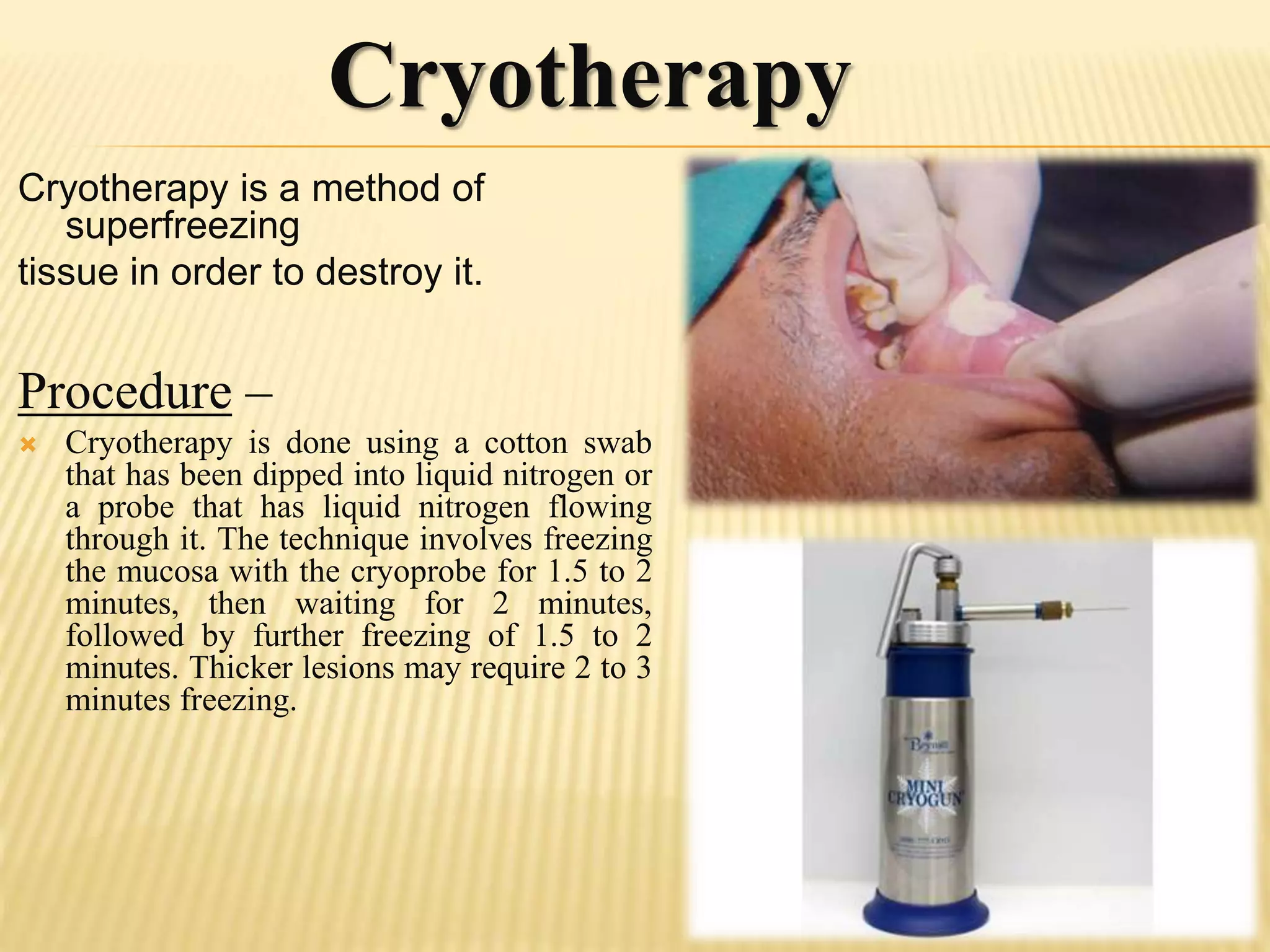
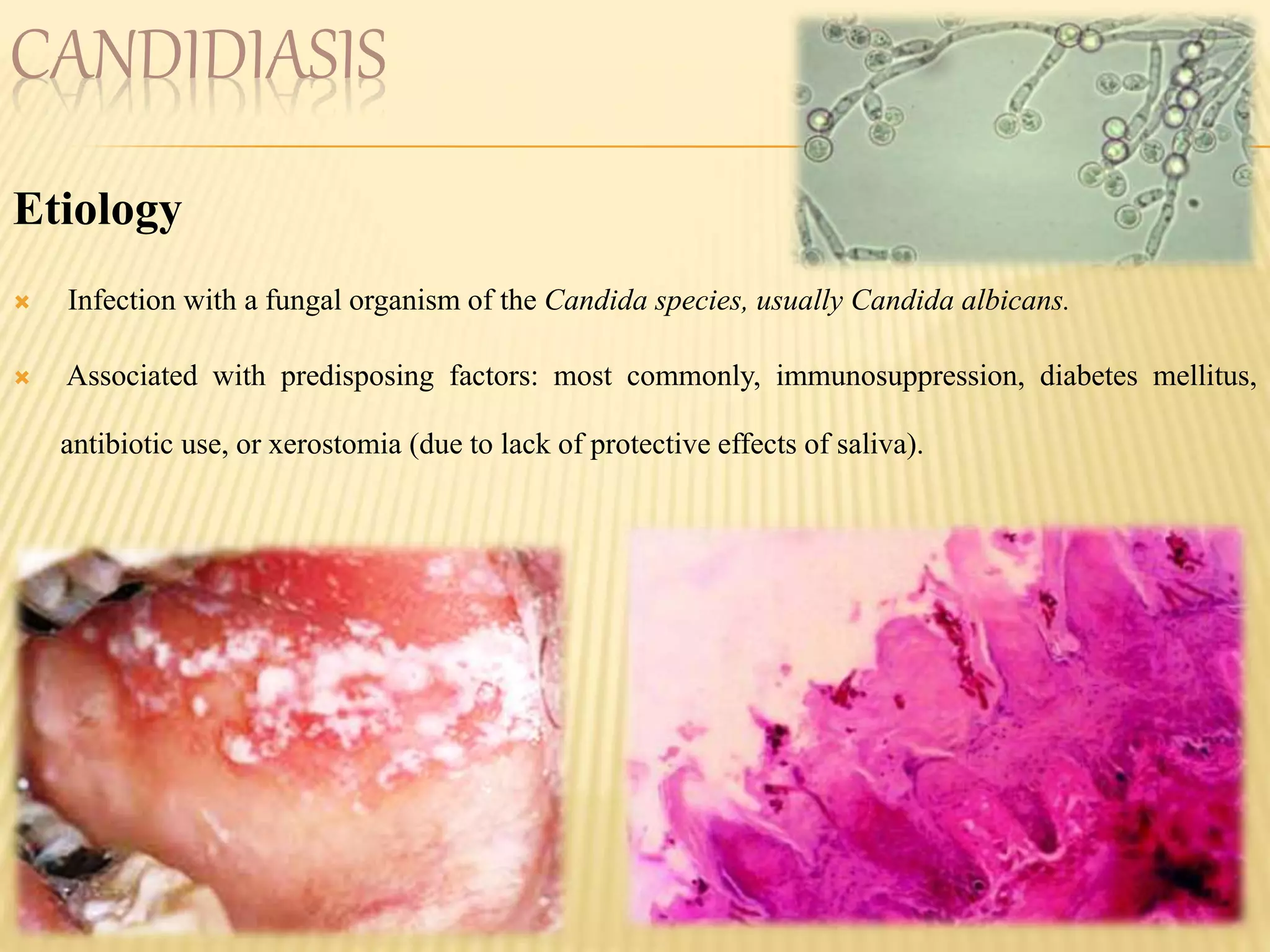
Etiology, clinical presentation, diagnosis, and treatment approaches for oral candidiasis.Describes OSMF as a chronic condition, its epidemiology and etiology.
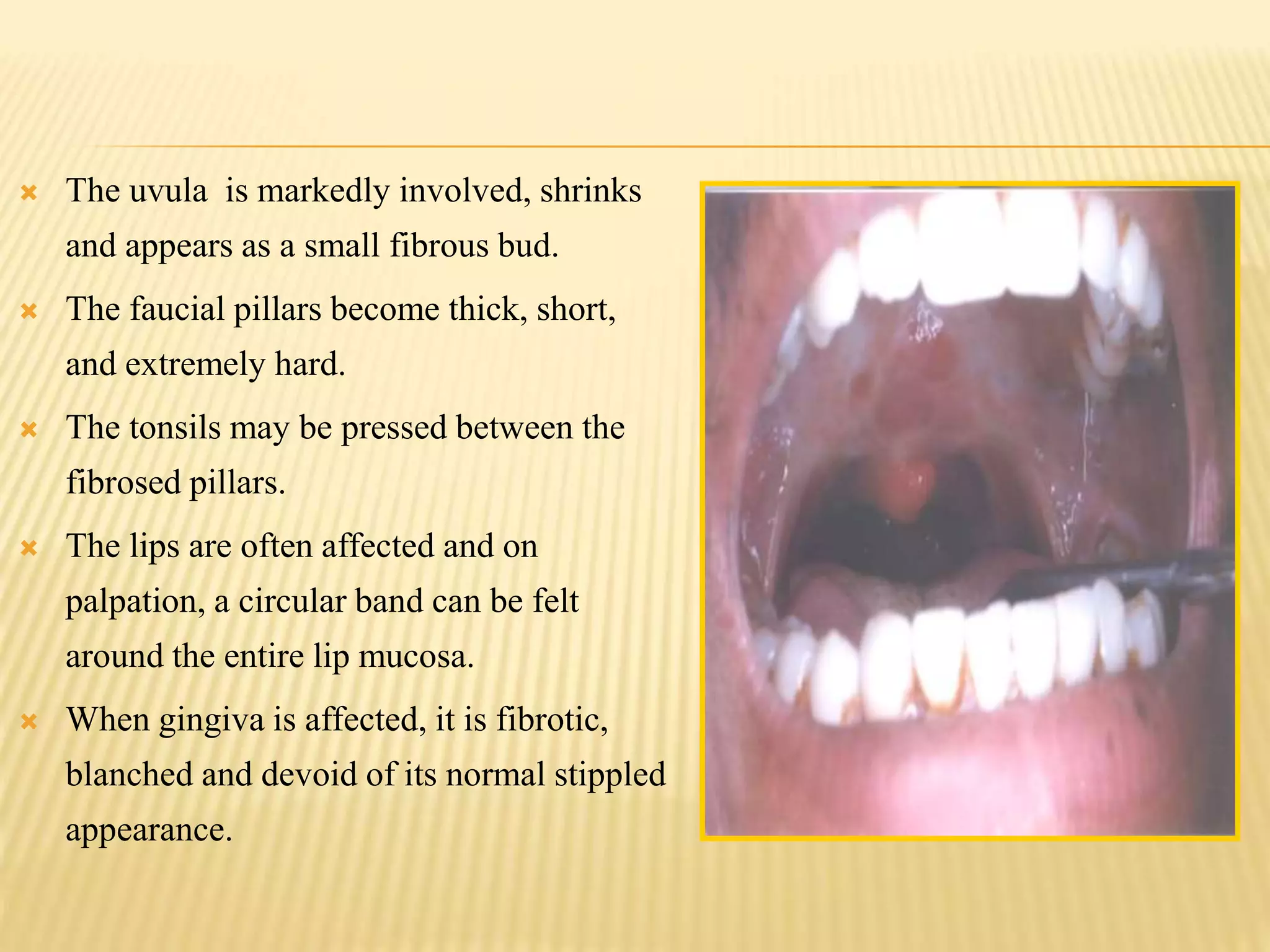
Symptoms and common oral sites affected by OSMF, including functional impacts.
Various stages of OSMF and their clinical implications along with recent classifications.
Diagnostic criteria including clinical features and histopathological findings for OSMF.
Overview of behavioral, non-surgical, and surgical management options for OSMF.Discussion on lichen planus, actinic keratosis, and other disorders related to oral cancer.
Techniques like ViziLite, toluidine blue, and exfoliative cytology for early detection.
New technologies like stem cell therapy and nanoparticle application for diagnosing oral cancer.
Importance of identifying PMD causative factors and monitoring for potential cancer transformation.
List of key textbooks and articles referenced throughout the presentation.
Closing remarks thanking the audience.
































































































