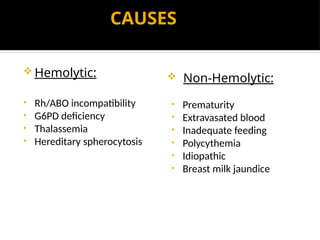
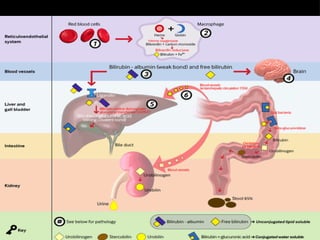
INTRODUCTION
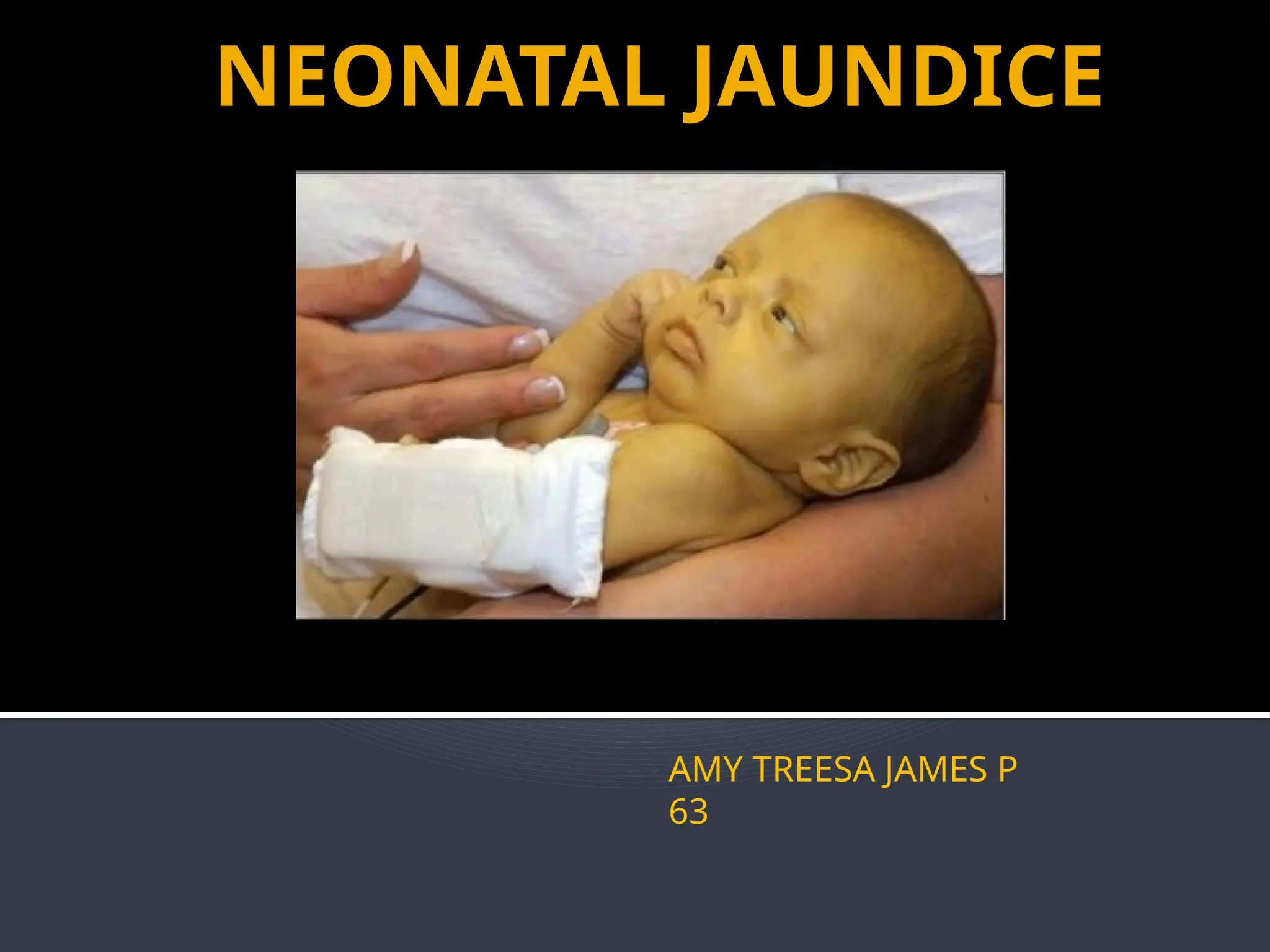
Important problemin the first week of life.
Dermal staining- yellow discoloration, cephalocaudal
direction.
High bilirubin levels- toxic to central nervous system &
cause neurological impairment.
Visual assessment- every 12hr during initial 3 to 5 days of
life, can be supplemented with TcB (Transcutaneous
bilirubinometry).
60% of term newborns-visibly jaundiced in 1st
week of life
but mostly benign.
5-10%-phototherapy or other therapeutic options.
3.
PHYSIOLOGICAL VS
PATHOLOGICAL JAUNDICE
Physiological Jaundice:
Physiological immaturity to handle increased bilirubin
production.
Visible jaundice-appears between 24-72 hrs.
TSB peaks in 3 days, then falls in term neonates.
Pathological Jaundice:
Appears within first 24 hrs of life.
Elevation of TSB level, exceeds 5mg/dL on first day, 10 mg/dL
in second day, 15 mg/dL thereafter.
Clinical jaundice-beyond 3 weeks.
Conjugated bilirubin.
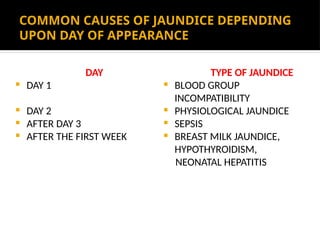
COMMON CAUSES OFJAUNDICE DEPENDING
UPON DAY OF APPEARANCE
DAY
DAY 1
DAY 2
AFTER DAY 3
AFTER THE FIRST WEEK
TYPE OF JAUNDICE
BLOOD GROUP
INCOMPATIBILITY
PHYSIOLOGICAL JAUNDICE
SEPSIS
BREAST MILK JAUNDICE,
HYPOTHYROIDISM,
NEONATAL HEPATITIS
7.
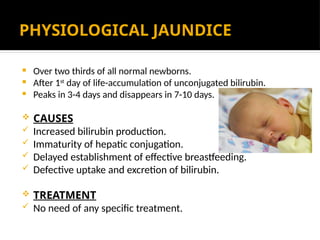
PHYSIOLOGICAL JAUNDICE
Overtwo thirds of all normal newborns.
After 1st
day of life-accumulation of unconjugated bilirubin.
Peaks in 3-4 days and disappears in 7-10 days.
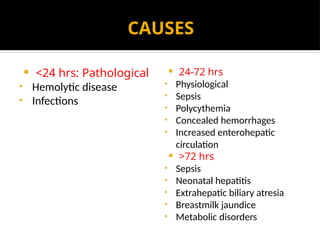
CAUSES
Increased bilirubin production.
Immaturity of hepatic conjugation.
Delayed establishment of effective breastfeeding.
Defective uptake and excretion of bilirubin.
TREATMENT
No need of any specific treatment.
9.
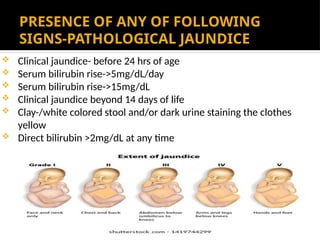
PRESENCE OF ANYOF FOLLOWING
SIGNS-PATHOLOGICAL JAUNDICE
Clinical jaundice- before 24 hrs of age
Serum bilirubin rise->5mg/dL/day
Serum bilirubin rise->15mg/dL
Clinical jaundice beyond 14 days of life
Clay-/white colored stool and/or dark urine staining the clothes
yellow
Direct bilirubin >2mg/dL at any time
10.
BREASTFEEDING JAUNDICE
• Exclusivelybreastfed- different
pattern of physiological
jaundice than artificially fed
babies.
• Inadequate breastfeeding.
• Appears: 24-72 hrs.
• Peaks: 5-15 days.
• Disappears: third week of life.
• 1/3rd
cases: mild jaundice in 3rd
week- persists into 2nd/3rd
month of life.
• Ensure optimum breastfeeding.
BREASTMILK JAUNDICE
• 2-4% cases-jaundice in excess
of 10 mg/dL beyond 3rd
/4th
week of life.
• Milk contain inhibitors of
conjugation(Pregnanediol, non
esterified long chain fatty acids)
• Diagnosis, if this is
unconjugated(mild
unconjugated
hyperbilirubinemia).
• Rule out other causes.
• Continue breastfeeding.
• Needs no treatment rarely
phototherapy.
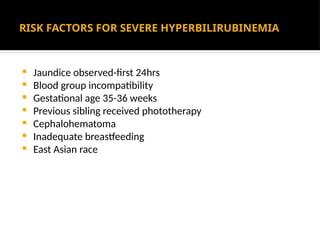
11.
RISK FACTORS FORSEVERE HYPERBILIRUBINEMIA
Jaundice observed-first 24hrs
Blood group incompatibility
Gestational age 35-36 weeks
Previous sibling received phototherapy
Cephalohematoma
Inadequate breastfeeding
East Asian race
12.
DANGERS OF HYPERBILIRUBINEMIA
KERNICTERUS
Unconjugated bilirubin can cross the immature Blood Brain Barrier
[BBB].
SYMPTOMS
• Lethargy
• Loss of Moro reflex
• Poor feeding
Intracranial involvement
• High pitched cry
• Bulging fontanel
• Seizures
• Opisthotonos
If Infant survives
• Choreoathetoid cerebral palsy
• Mental retardation
• Paralysis of upward gaze
• High-frequency hearing impairment
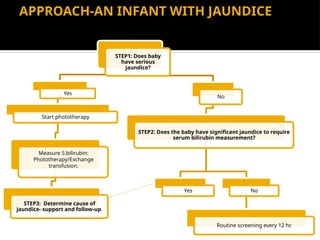
APPROACH-AN INFANT WITHJAUNDICE
visual assessment every 12 hrs, first 3-5 days ; TRANSCUTANEOUS IF AVAILABLE.
STEP1: Does baby
have serious
jaundice?
Yes
Start phototherapy
Measure S.bilirubin:
Phototherapy/Exchange
transfusion.
STEP3: Determine cause of
jaundice- support and follow-up.
No
STEP2: Does the baby have significant jaundice to require
serum bilirubin measurement?
Yes No
Routine screening every 12 hr.
15.
INVESTIGATIONS
FIRST LINE
•Total serum bilirubin.
• Blood groups of mother and baby.
• Peripheral smear: Evidence of hemolysis.
SECOND LINE
• Direct Coombs test: Antibody coating on fetal RBC.
• Hematocrit: Decreased in hemolysis.
• Reticulocyte count: Increased in hemolysis
• G6PD levels.
• Others: Sepsis screen, thyroid function test, rule out
other genetic enzyme deficiencies.
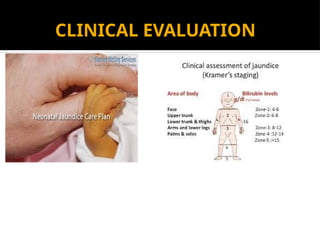
16.
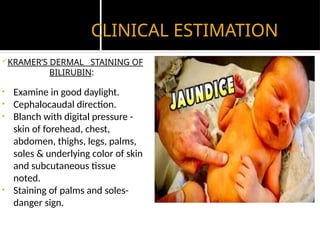
CLINICAL ESTIMATION
KRAMER’S DERMALSTAINING OF
BILIRUBIN:
• Examine in good daylight.
• Cephalocaudal direction.
• Blanch with digital pressure -
skin of forehead, chest,
abdomen, thighs, legs, palms,
soles & underlying color of skin
and subcutaneous tissue
noted.
• Staining of palms and soles-
danger sign.
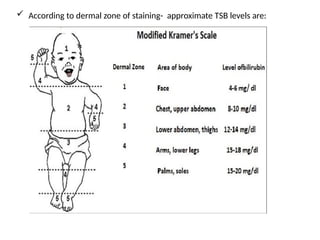
17.
According todermal zone of staining- approximate TSB levels are:
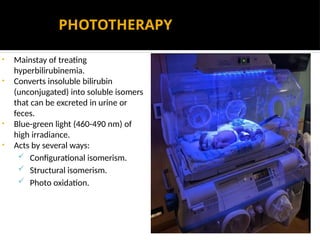
PHOTOTHERAPY
• Mainstay oftreating
hyperbilirubinemia.
• Converts insoluble bilirubin
(unconjugated) into soluble isomers
that can be excreted in urine or
feces.
• Blue-green light (460-490 nm) of
high irradiance.
• Acts by several ways:
Configurational isomerism.
Structural isomerism.
Photo oxidation.
24.
TYPES OF PHOTOTHERAPYLIGHTS
Fluorescent lamps of different colors and shapes(CFLs)
Halogen bulbs
High intensity LEDs (blue)-long life, high irradiance
Fibro-optic light sources
25.
PROCEDURE
Ensure optimumroom temperature: 25-28 degree Celsius.
Keep the baby in a cot/ bassinet/ incubator/ radiant warmer.
Remove all clothes of baby except diaper. Expose maximal surface
area of body. Avoid blocking of light by any equipment.
Cover baby’s eyes with an eye patch.
Keep the distance between baby and light 30-45 cms.
Ensure optimum breastfeeding. Minimize interruption of
phototherapy during feeding sessions or procedures.
Monitor temperature of baby every 2-4 hours.
Measure TSB levels every 12-24 hrs.
Discontinue once two TSB values 12 hours apart fall below current
age-specific cut offs.
Monitor for rebound rise within 24 hrs after stopping
phototherapy.
EXCHANGE TRANSFUSION
DoubleVolume Exchange Transfusion(DVET) should be done if TSB
levels reach to age specific cut-off for ET or signs of bilirubin
encephalopathy is seen.
INDICATIONS
Cord bilirubin: 5mg/dL or more.
Cord Hb is 10mg/dL or less.
ET performed by pull and push technique through umbilical venous
route.
Umbilical catheter should be inserted.


![DANGERS OF HYPERBILIRUBINEMIA
KERNICTERUS
Unconjugated bilirubin can cross the immature Blood Brain Barrier
[BBB].
SYMPTOMS
• Lethargy
• Loss of Moro reflex
• Poor feeding
Intracranial involvement
• High pitched cry
• Bulging fontanel
• Seizures
• Opisthotonos
If Infant survives
• Choreoathetoid cerebral palsy
• Mental retardation
• Paralysis of upward gaze
• High-frequency hearing impairment](https://image.slidesharecdn.com/neonataljaundice-250225142033-c17b9258/85/Neonatal-Jaundice-pptx-pediatrics-presentation-12-320.jpg)

![CUT-OFFS FOR TREATMENT IN PRETERMS:
GESTATION
(COMPLETED WEEKS)
PHOTOTHERAPY
[TSB-mg/dL]
EXCHANGE
TRANSFUSION
[TSB-mg/dL]
<28 weeks 5-6 11-14
28-29 weeks 6-8 12-14
30-31 weeks 8-10 13-16
32-33 weeks 10-12 15-18
34 weeks 12-14 17-19](https://image.slidesharecdn.com/neonataljaundice-250225142033-c17b9258/85/Neonatal-Jaundice-pptx-pediatrics-presentation-18-320.jpg)