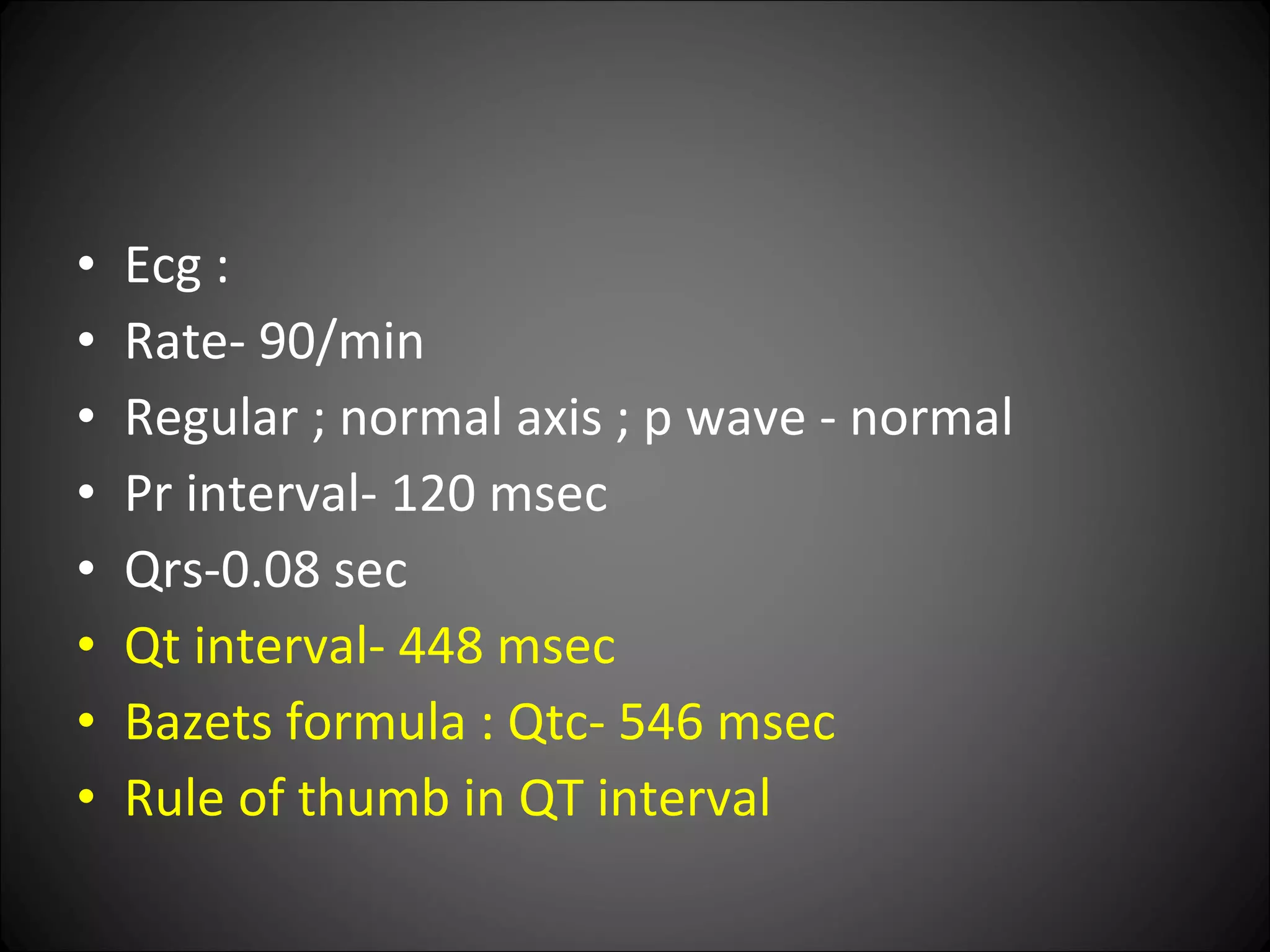
A 17-year-old female presented with seizures for the past 6 months. On examination, she was found to have hypocalcemia with a serum calcium level of 5.7 mg/dl. Further workup revealed low levels of parathyroid hormone, indicating hypoparathyroidism as the cause of her hypocalcemia and seizures. Brain CT and EEG were normal. She was started on calcium and vitamin D supplementation, which improved her symptoms and lab abnormalities.
















![Serum calcium: 5.7 mg/dl[normal-8-10]](https://image.slidesharecdn.com/acaseofseizure-110125051657-phpapp01/75/An-Interesting-Case-of-Seizure-18-2048.jpg)

![Serum calcium: 5.7 mg/dl[normal-8-10] Serum albumin : 3.8 gm /dl Ionised calcium- 0.452 mmol/l[ 1.16-1.32] Unionised calcium- 0.458 mmol/l Serum Phosphorus : 6.2 (2.5 – 4.5 mmol/dl ) Serum PTH : 5.2pg/ml ( 8-51 pg/ml ) 24 Hrs urine Calcium : 7mg/L (< 300mg/day) Sr. Alkaline Phosphatase : 37 IU/l ( 33-100)](https://image.slidesharecdn.com/acaseofseizure-110125051657-phpapp01/75/An-Interesting-Case-of-Seizure-20-2048.jpg)


![Serum magnesium: 2.1 mg/dl[1.7 to 2.55] History didn’t suggest any cause that could lead to acquired hypoparathyroidism No significant history in family members No facial dysmorphism ; short stature. Skin –No hyperpigmentation / vitiligo / muco-cutaneus candidiasis / abscess n scars / eczematous changes. Thyroid profile :Normal](https://image.slidesharecdn.com/acaseofseizure-110125051657-phpapp01/75/An-Interesting-Case-of-Seizure-23-2048.jpg)








![[Idiopathic hypoparathyroidism, a syndrome with various clinical expressions: analysis of 10 cases] Rev Med Chil. 1989 Jun;117(6):647-52. Abstract We report 10 patients with primary hypoparathyroidism. Age at onset varied from 7 months to 52 years (mean 28); 7 were female. Diagnosis was established at a mean of 4.1 years after the appearance of clinical manifestations. Unexplained hypocalcemia (mean 5.3 mg/dl) and hyperphosphatemia (mean 6.4 mg/dl) were present in all patients. Prevalent symptoms included tetany (9 patients), seizures (5) and hypocalcemic cataracts (4 ). Clinical manifestations may be grouped into 5 types 1) tetany; 2) seizures; 3) other neurologic disorders (basal ganglia calcification, pseudotumor of the brain, ataxia, nystagmus, hypertonus, paresis); 4) disorders of the lens including fully developed cataracts and 5) skin alterations like psoriasis and others. Some of these run on acute course (seizures, tetany), others a subacute one (skin alterations) while others are rather chronic (cataract and other neurologic disorders ). Seizures and electroencephalographic disorders predominate in younger patients while tetany is more prevalent in older subjects.](https://image.slidesharecdn.com/acaseofseizure-110125051657-phpapp01/75/An-Interesting-Case-of-Seizure-33-2048.jpg)








![Hereditary hypoparathyroidism May occur without any other endocrinological and dermatological manifestations. Manifest within first decade or later. Syndrome associated with hypopara thyroidism Di George syndrome[ DSG1-chromosome-22. DSG1-Chromosome10]. Kenney- Caffey syndrome: hypo parathyroidism, short stature, osteo sclerosis, thick cortical bones. Sanjad-Sakati synd: growth failure and dysmorphic features. Basal ganglia calcification and extra pyramidal symptoms are more common and earlier in onset.](https://image.slidesharecdn.com/acaseofseizure-110125051657-phpapp01/75/An-Interesting-Case-of-Seizure-42-2048.jpg)









![TREATMENT Vitamin-D - 40000 to 1,20,000 iu/day[ 1-3 mg /day] combined with elemental calcium is satisfactory. Calcitriol- 0.5 to 1 micro gram/day. They do not reverse the lowered urinary calcium reabsorption. Thiazide diuretics lower urinary calcium in hypoparathyroid pts on vit-D.](https://image.slidesharecdn.com/acaseofseizure-110125051657-phpapp01/75/An-Interesting-Case-of-Seizure-52-2048.jpg)
![HYPOMAGNESEMIA Levels less than 0.4 mmol/l[ 0.8 meq/l] Reduced PTH secretion or reduced response to PTH Severe hypomagnesemia is paradoxically associated with low PTH level. Cause unknown. Serum phosphate levels are usually not elevated. When magnesium is repleted restoration of PTH levels may preceed serum calcium by several days. Treatment- IV magnesium.](https://image.slidesharecdn.com/acaseofseizure-110125051657-phpapp01/75/An-Interesting-Case-of-Seizure-53-2048.jpg)













































































































