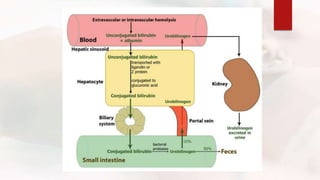
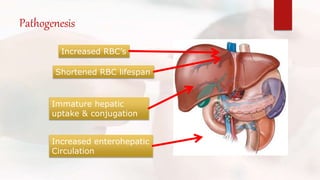
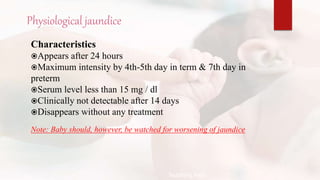
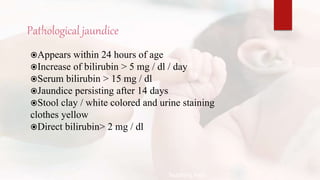
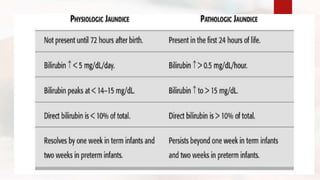
The document discusses neonatal jaundice, a condition characterized by high bilirubin levels resulting in yellowing of the skin and eyes in newborns. It outlines the incidence, types (physiological and pathological), causes, clinical assessment, diagnosis, and management strategies such as phototherapy and exchange transfusion. Additionally, it highlights the importance of early detection and treatment to prevent complications like kernicterus.