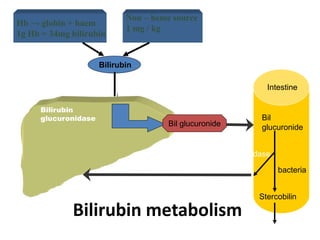
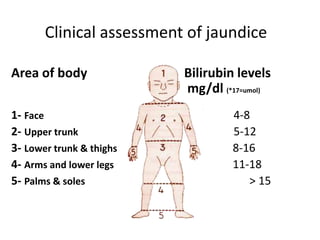
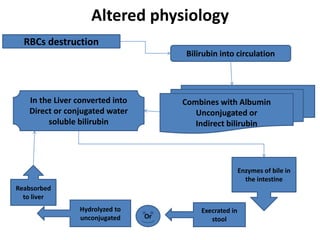
This document discusses neonatal jaundice (hyperbilirubinemia), which refers to an excessive level of bilirubin in the blood that causes jaundice. It notes that physiological jaundice occurs in 50-60% of term and 80% of preterm neonates, but significant jaundice affects only 6% of term babies. The document describes the causes, risk factors, diagnosis, and treatment of pathological jaundice, including phototherapy and exchange transfusion. Nursing considerations for babies receiving phototherapy focus on monitoring temperature and fluid intake to prevent complications during therapy.