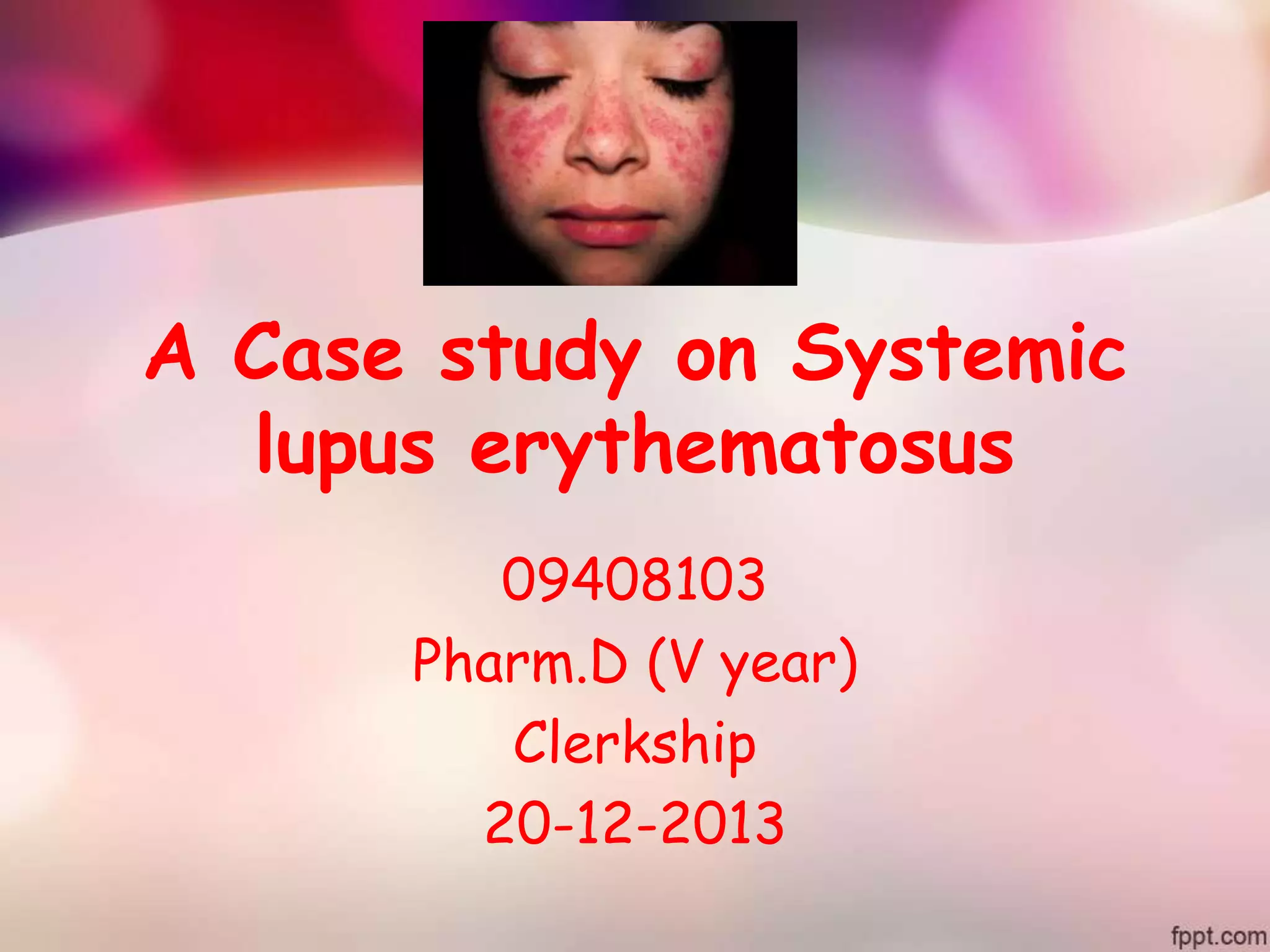
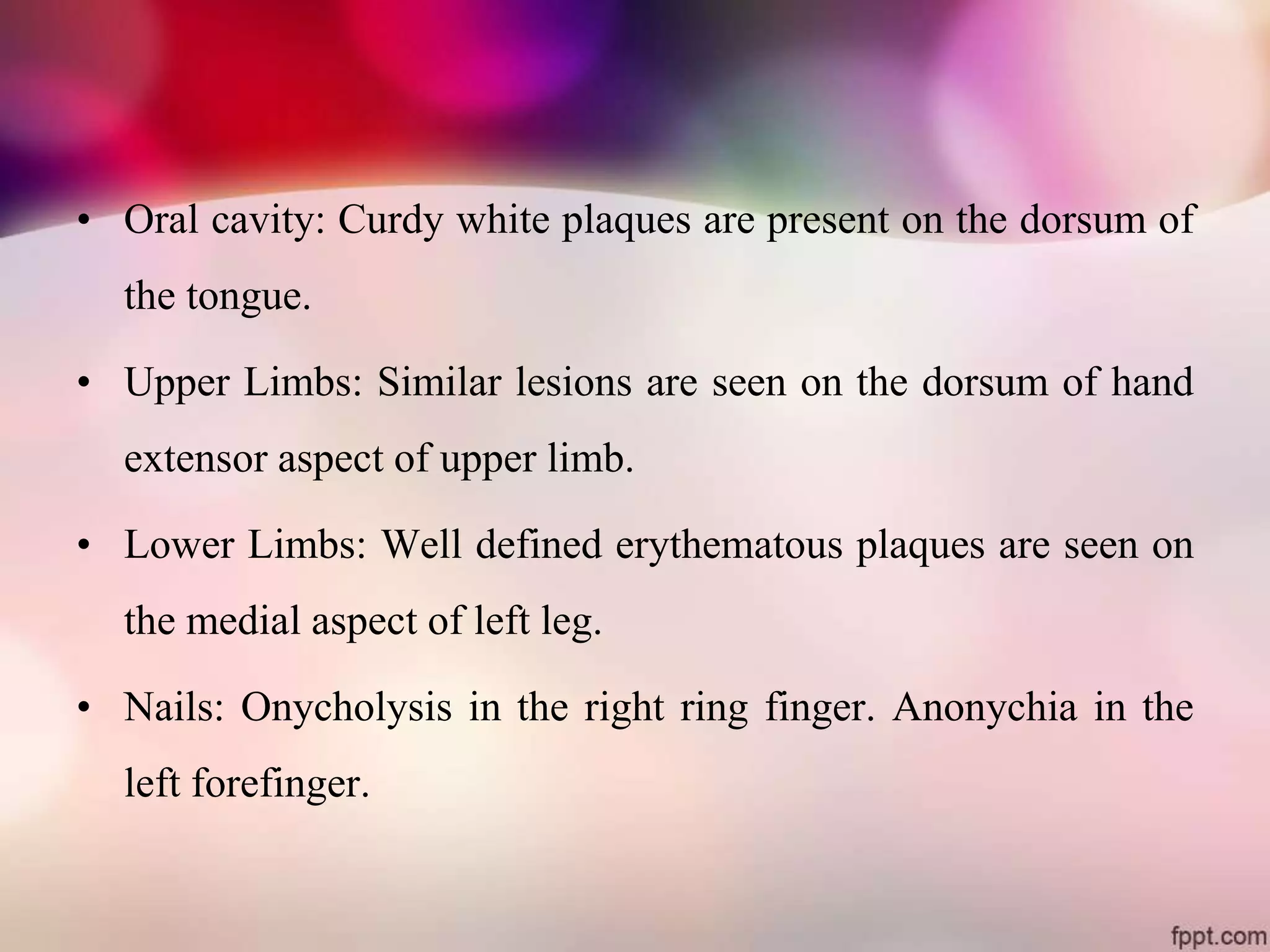
A 45-year-old female patient with a history of systemic lupus erythematosus (SLE) was admitted to the hospital with a cough producing sputum for 8 days and fever for 5 days. On examination, the patient exhibited rashes, lesions, and nail abnormalities consistent with SLE. Laboratory tests showed slightly elevated albumin and globulin levels. She was diagnosed with SLE and treated with corticosteroids, hydroxychloroquine, proton pump inhibitors, and other medications. The patient was counseled on adherence to treatment, lifestyle changes like avoiding sunlight, and reporting any adverse effects.