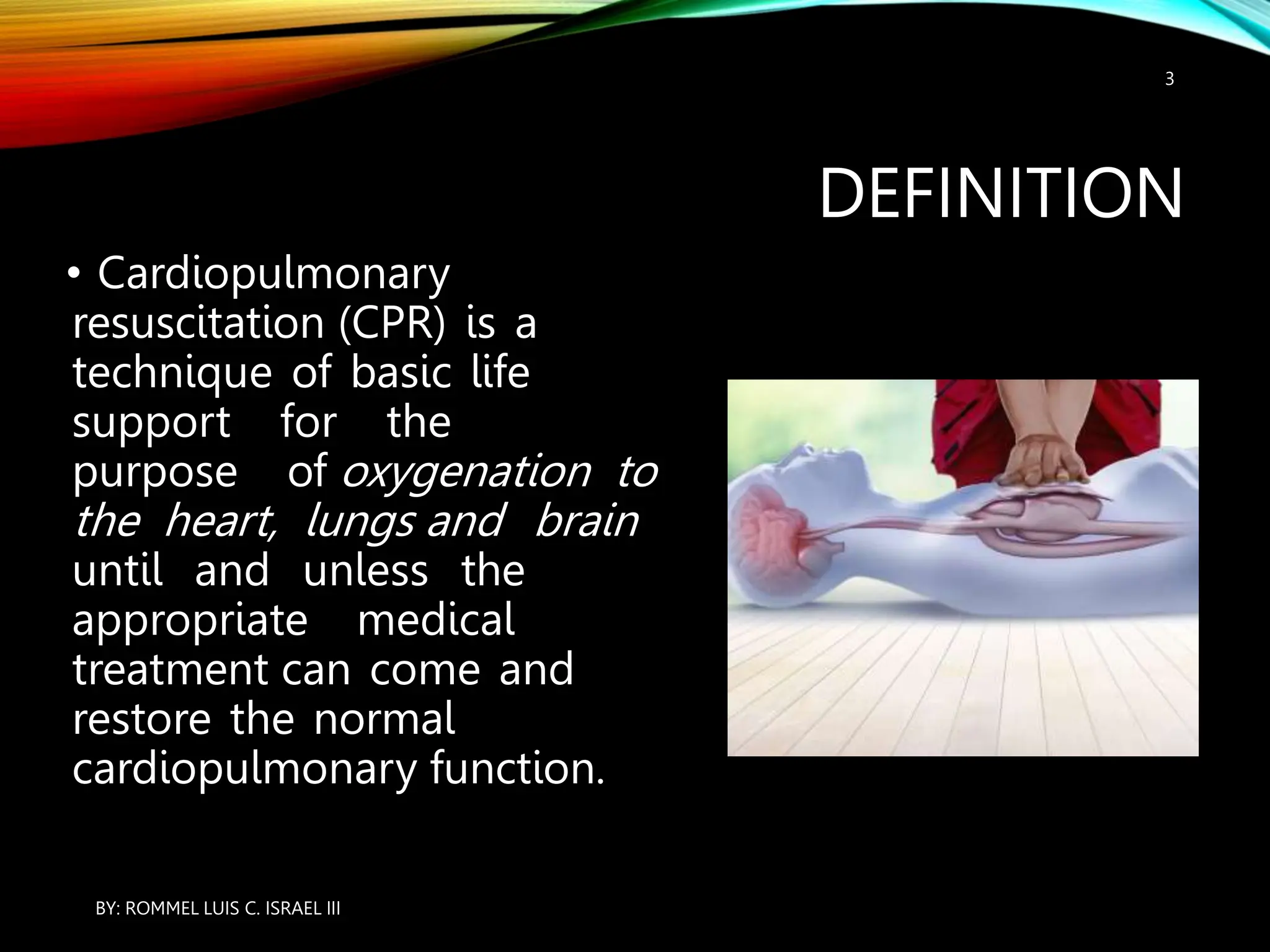


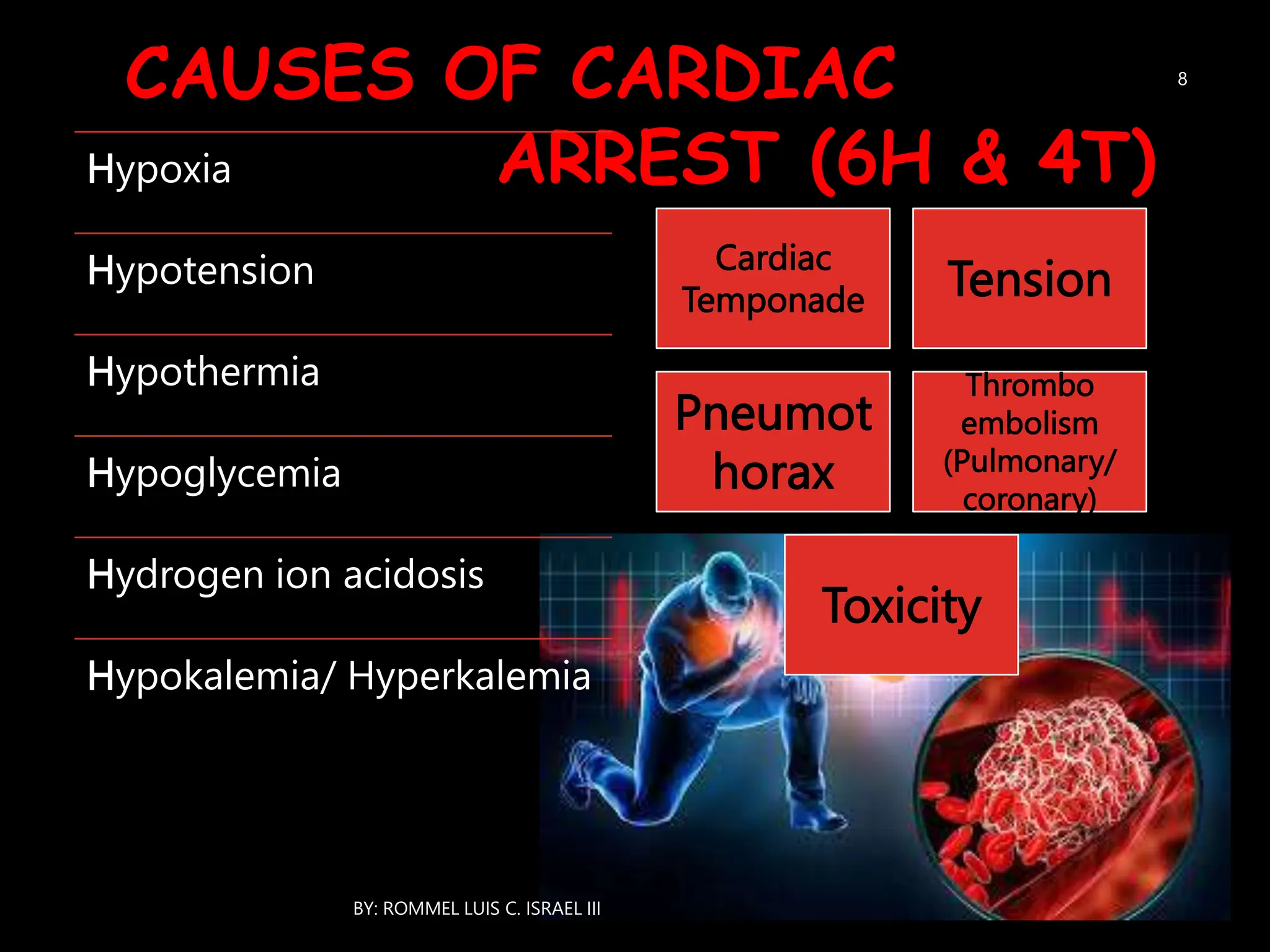





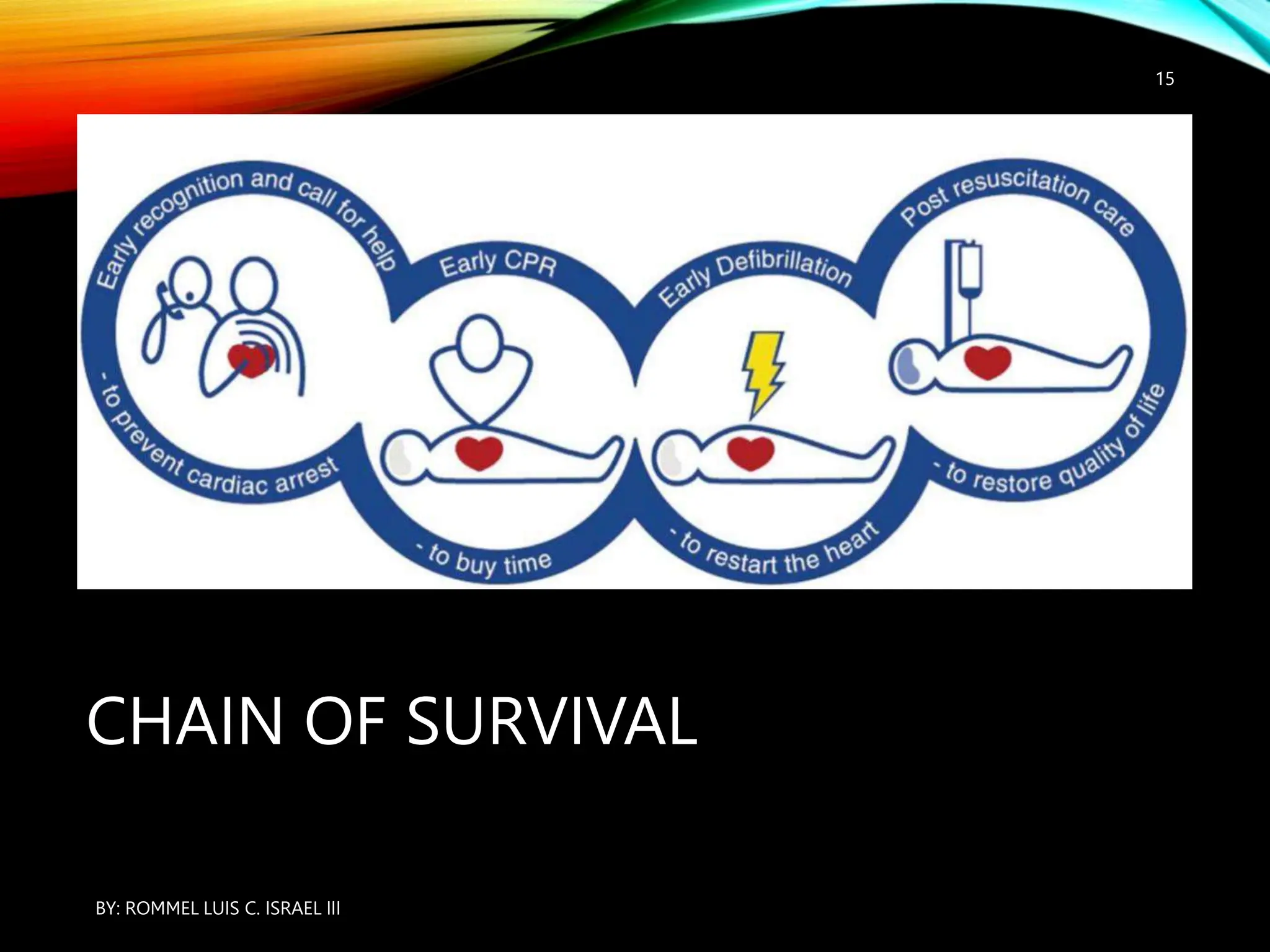
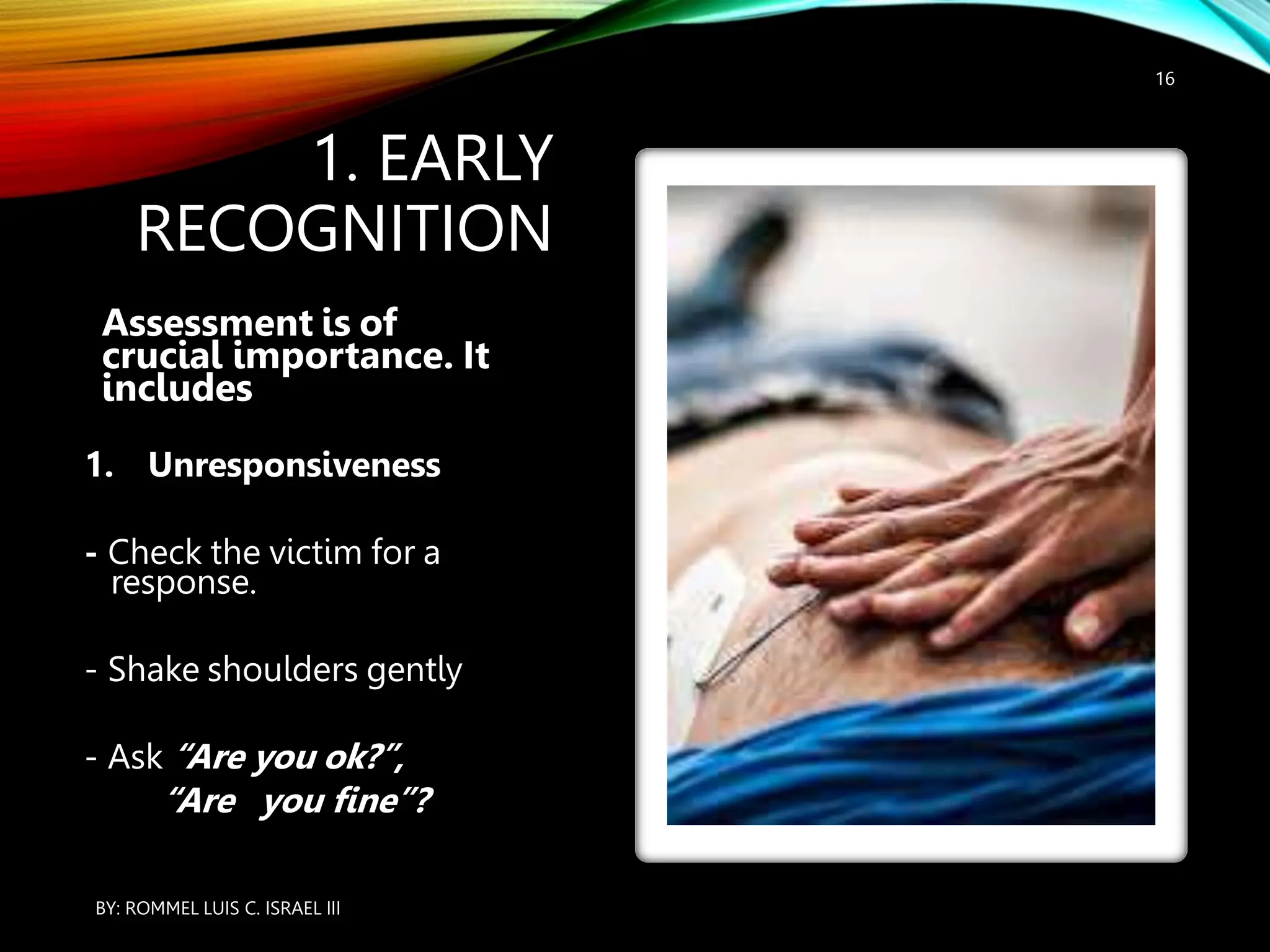

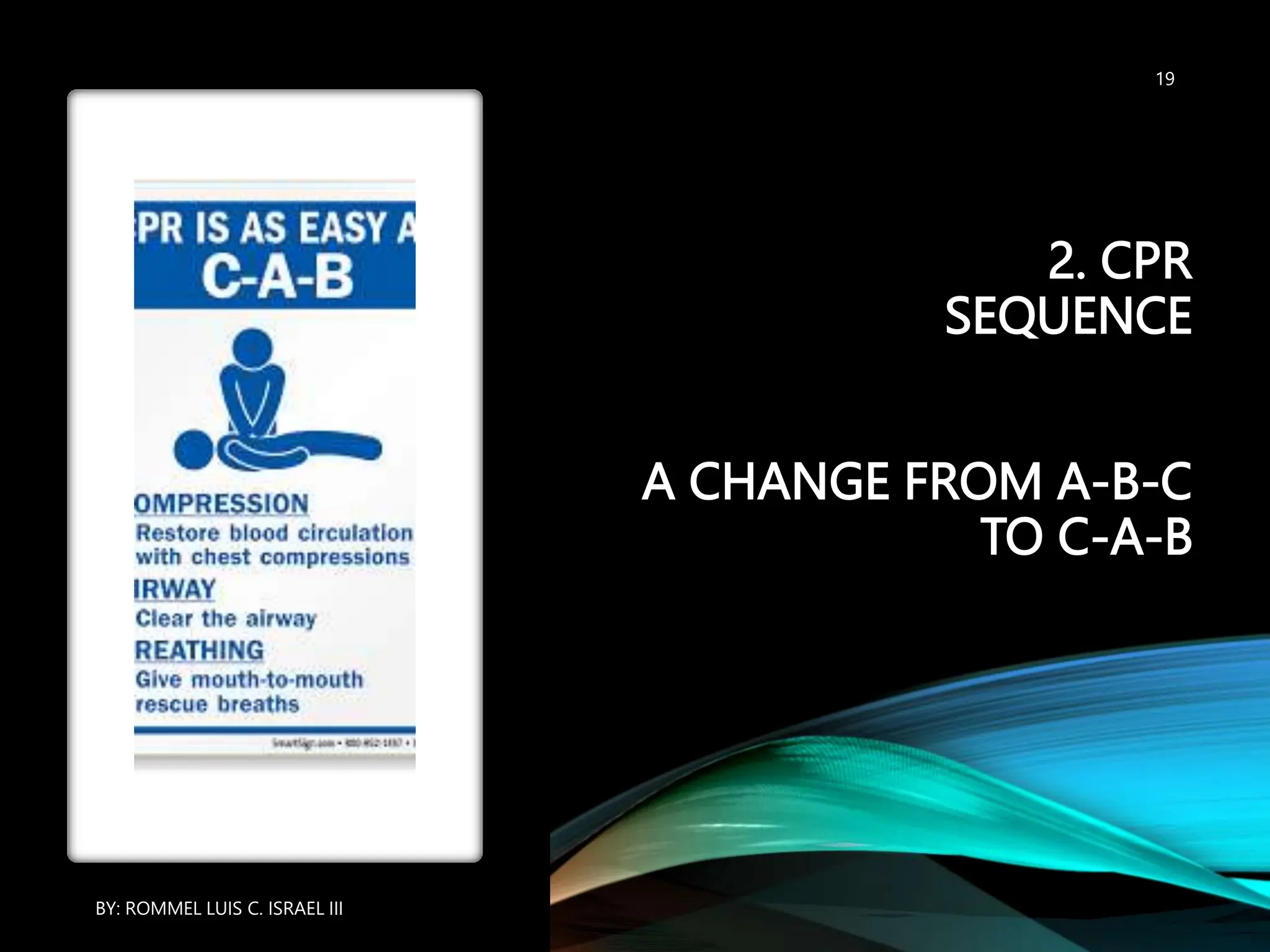

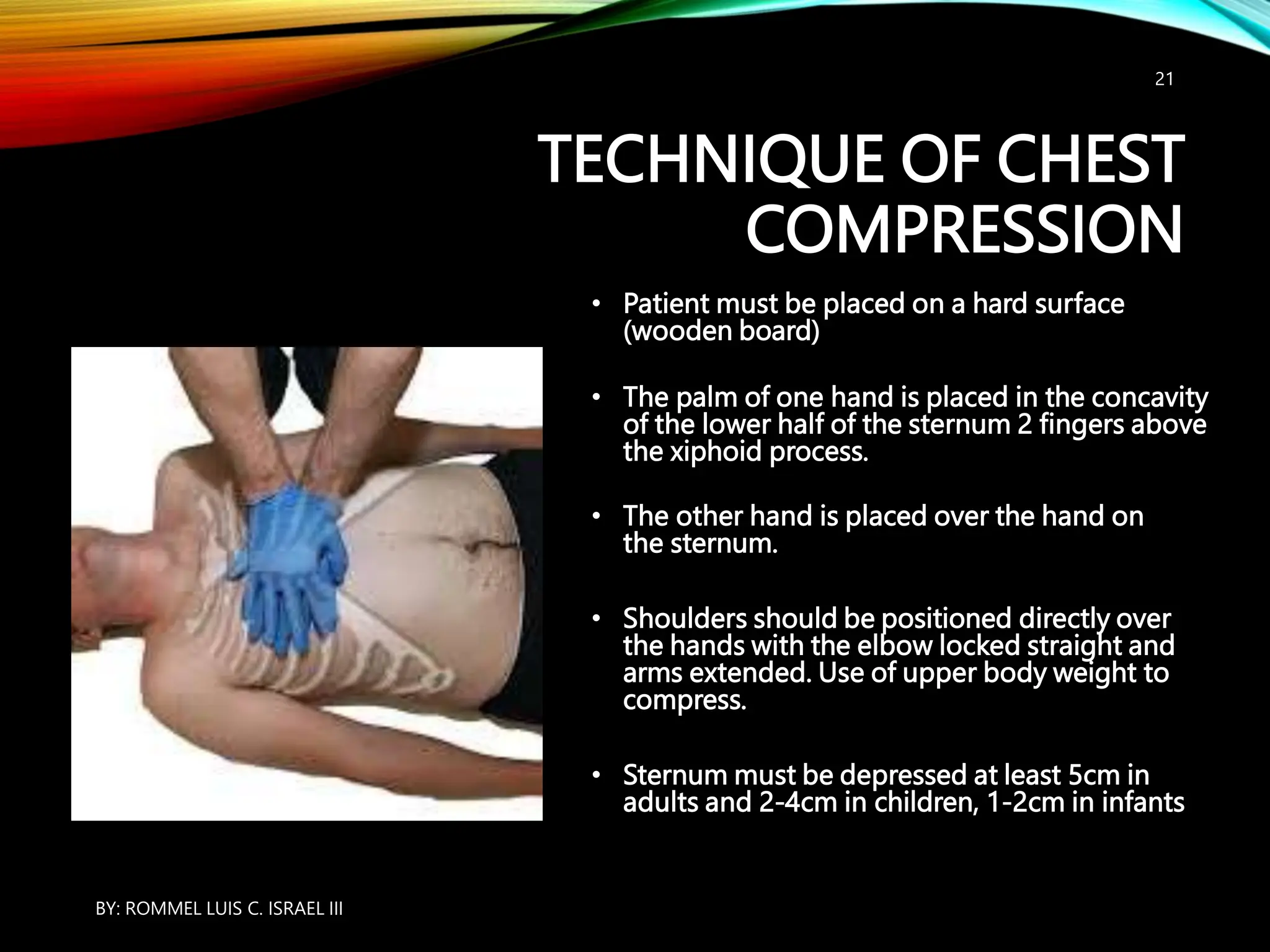

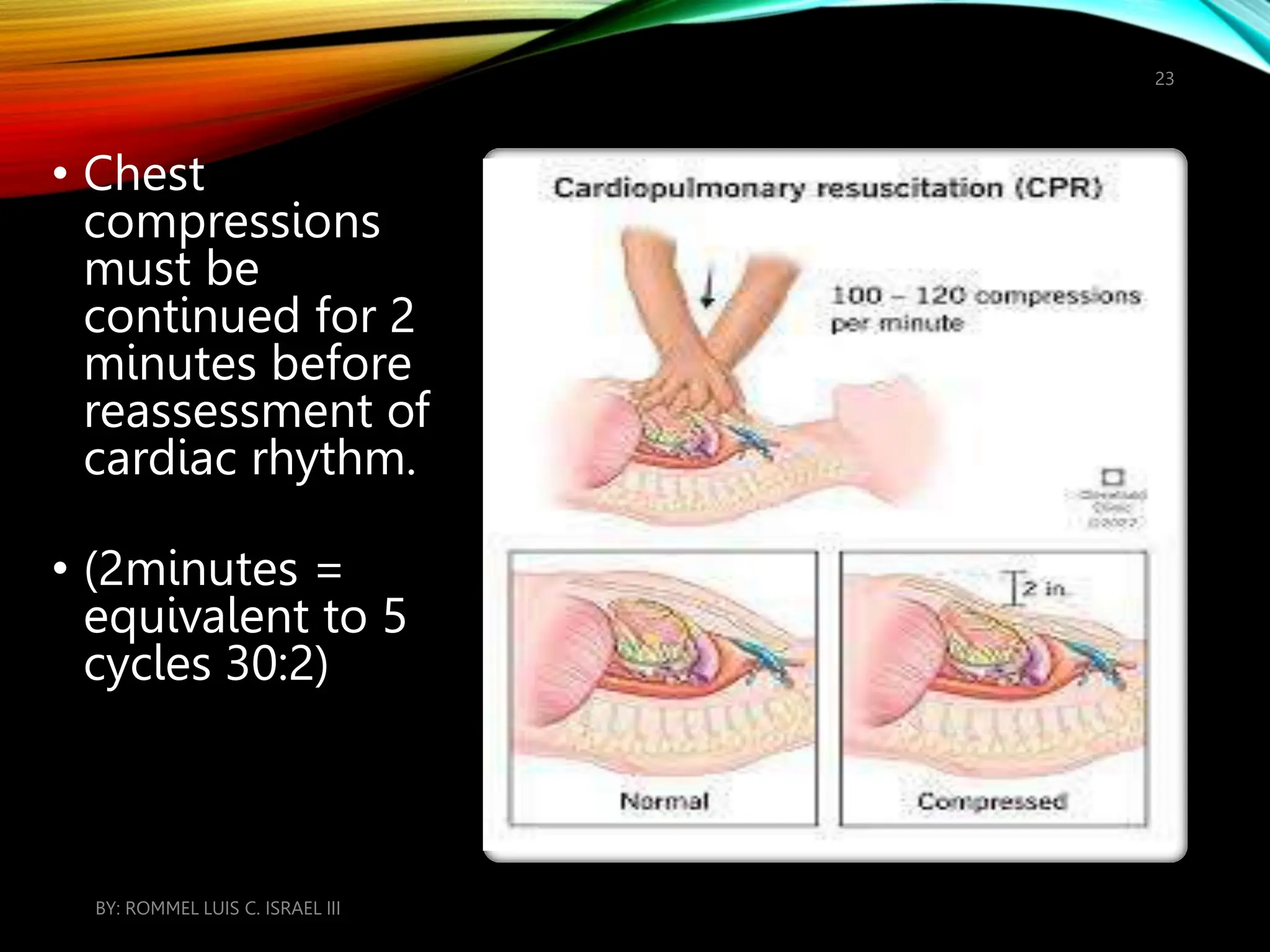

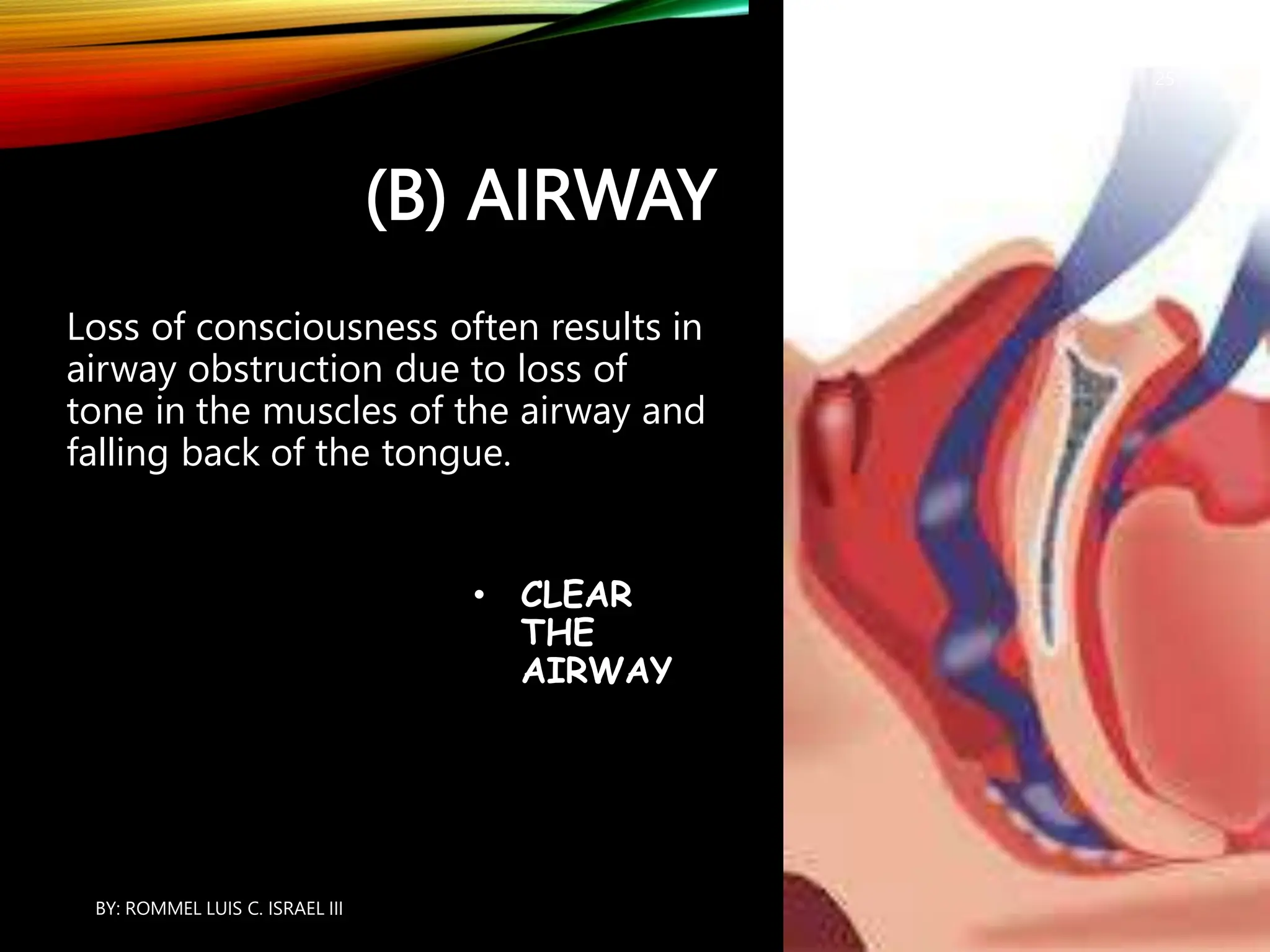

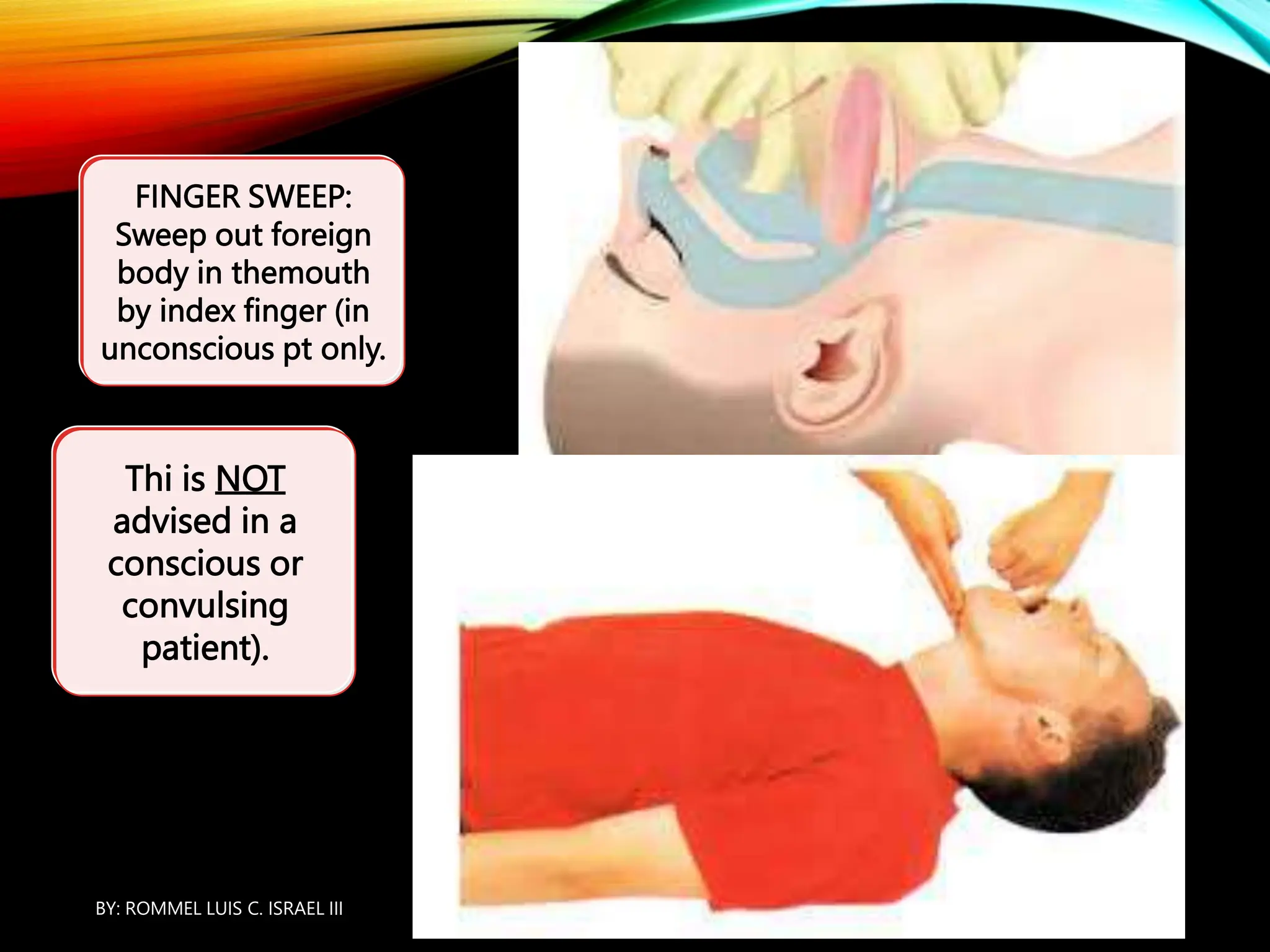

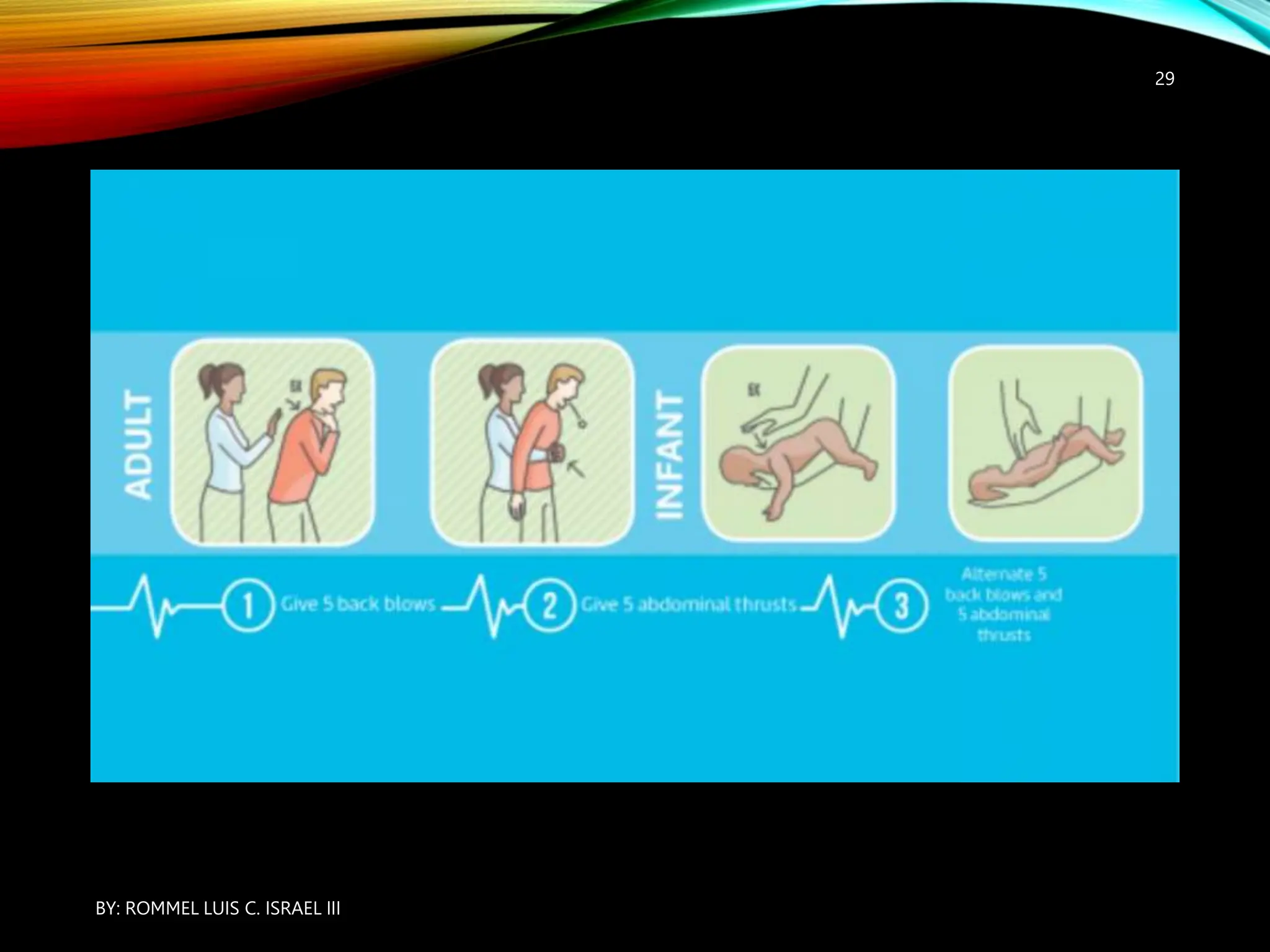














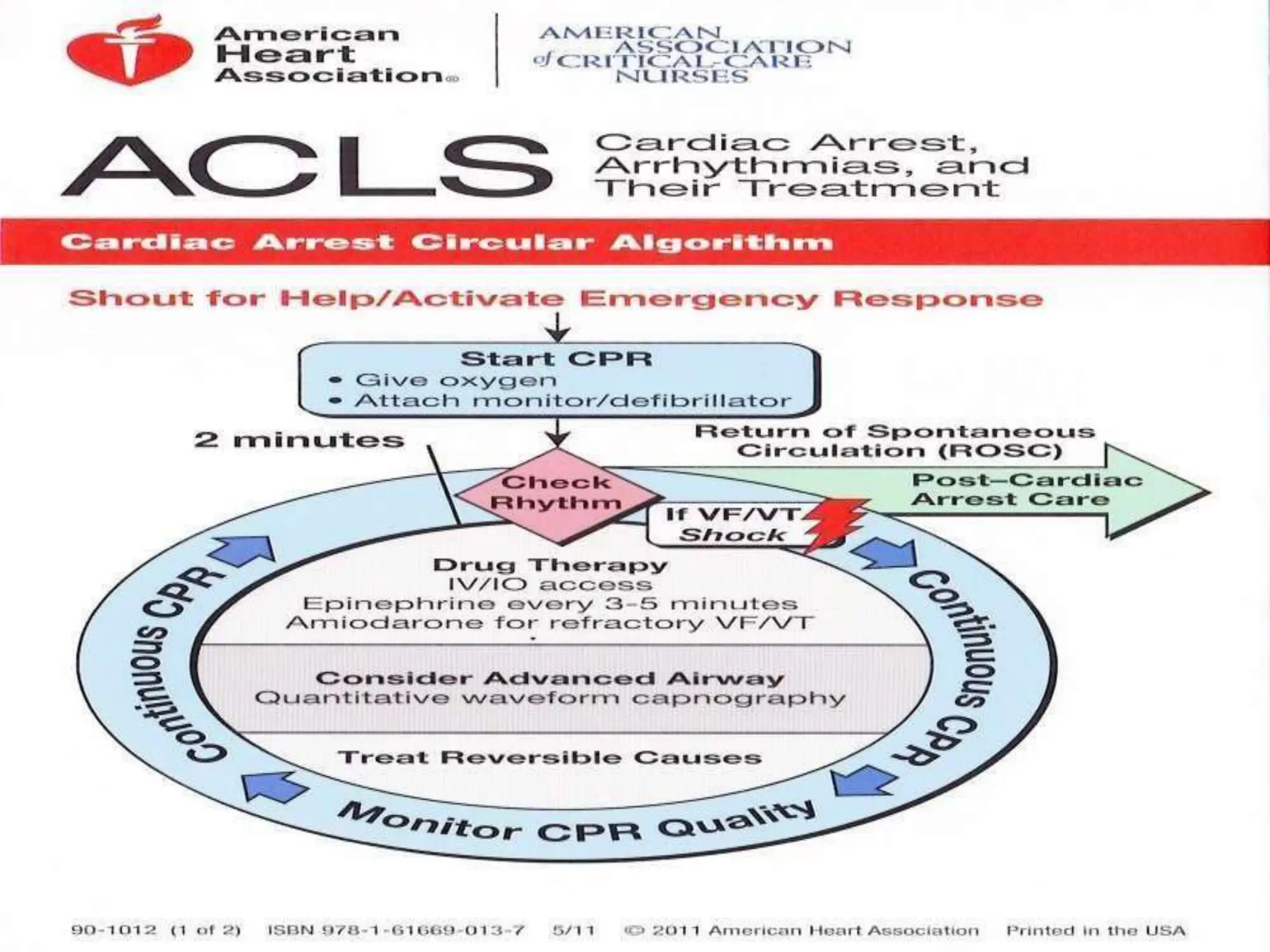




























The document discusses Cardiopulmonary Resuscitation (CPR) including its definition, purpose, indications, and how it works. CPR involves restoring circulation through chest compressions and restoring breathing through rescue breathing. It describes the basic steps of CPR including the CAB sequence of clearing the airway, giving breaths, and performing chest compressions. The document also discusses advanced life support techniques, use of an automated external defibrillator, drugs administered during CPR, and indications for terminating resuscitation efforts.























































































