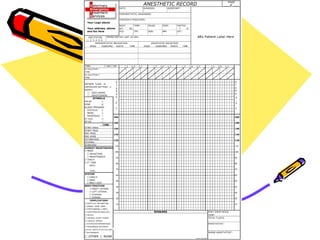
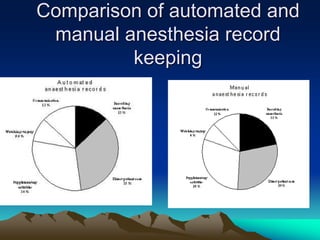
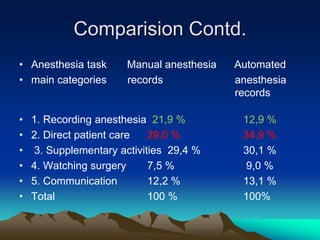
This document discusses the history and importance of medical records, particularly anesthesia records. It notes that medical records have existed for thousands of years, becoming more standardized over time. Maintaining thorough and accurate anesthesia records is important for patient safety, medico-legal purposes, research, and demonstrating the quality of care provided. The document compares manual and computer-based methods of record keeping and outlines the key information that should be included in pre-operative, intra-operative, and post-operative anesthesia records.


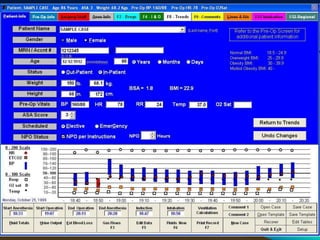

![PREOPERTIVE INFORMATION
• Patient Identity
– Name / I.D No. / gender
– Demographic details
– Date of birth / Age
• Assessment and risk factors
– Date of assessment
– Assessor, where assessed
– Weight (kg), [height (m) optional]
– Basic vital signs (BP, HR)
– Medication, incl. contraceptive drugs
– Past History of Illness, Family History & Allergies](https://image.slidesharecdn.com/anaesthesiarecordkeeping-240121095828-58635af4/85/Anaesthesia-file-done-Record-keeping-ppt-38-320.jpg)
































![Chapter 2 pre_anesthetic_evaluation_presentation_1_for_students [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/chapter2preanestheticevaluationpresentation1forstudentsautosaved-210422073416-thumbnail.jpg?width=640&height=640&fit=bounds)























































