























































































































































































































































![2. Maintaining
electrolyte and
acid-base balance
a. Monitor and replace
serum electrolytes
ordered.
Evaluate for signs and symptoms of
hyperkalemia and notify the physician of value
above 5.5 mg/L.
Watch for ECG changes like tall T waves; wide
QRS complex; depressed ST segment.
Administer sodium bicarbonate or glucose and
insulin to shift potassium into the cells, as
ordered.
Administer cation exchange resin (sodium
polystyrene sulfonate [Kayexalate]) orally or
rectally to provide more prolonged correction of
elevated potassium, as ordered.
Administer aluminum hydroxide for
hyperphosphatemia
Instruct patient about the importance of following
the prescribed diet, avoiding foods high in
potassium.
Prepare for dialysis when a rapid lowering of
potassium is needed.](https://image.slidesharecdn.com/fluidanelectrolytes2024-rommelisrael-240827132024-ab052bad/75/FLUID-AN-ELECTROLYTES-UPDATED-COPY-pptx-257-2048.jpg)











































































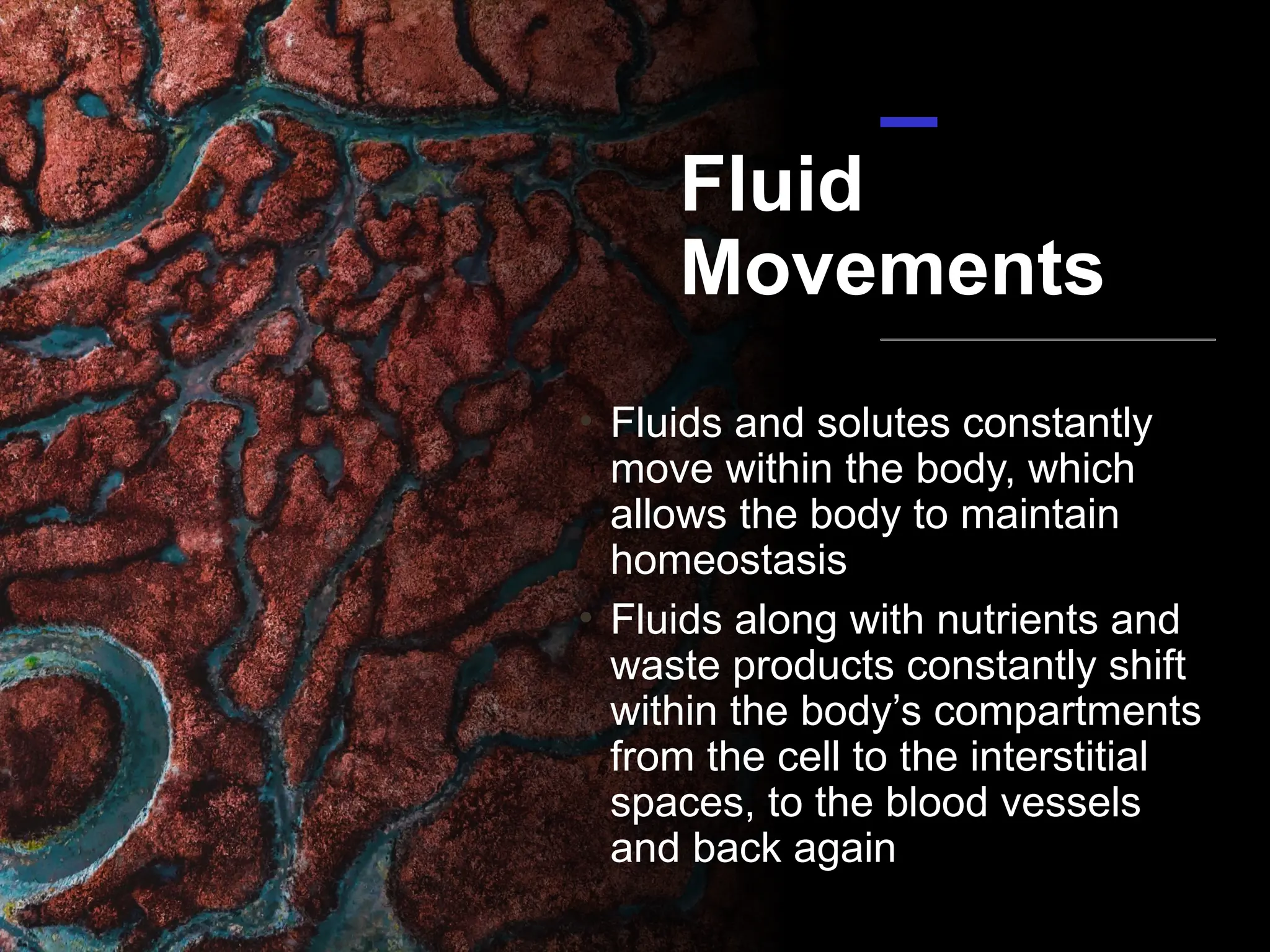
The document discusses the importance of fluids and electrolytes in the human body, highlighting their roles in cellular function, temperature regulation, and nutrient transport. It explains homeostasis, the body's feedback mechanisms, and fluid replacement therapy methods, specifically focusing on the renin-angiotensin-aldosterone system and the regulation of water balance. Additionally, it covers fluid assessment, potential imbalances, and the nursing interventions required to manage fluid deficits or excesses.












![Fluid and electrolyte imbalance [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/btwa8l8ysletobnf0row-signature-f3069b4a7063ad7d39b14083d6e8689bac823dbcf19c3f5cb443fa8d754857b7-poli-171013171124-thumbnail.jpg?width=640&height=640&fit=bounds)










































































