Cardiac tamponade is a life-threatening condition where fluid rapidly accumulates in the pericardial space, preventing the heart from filling properly. It can be caused by many acute or chronic conditions. Physical exam findings include elevated jugular venous pressure, low blood pressure that drops further with inspiration (pulsus paradoxus), and muffled heart sounds. Diagnosis is confirmed with echocardiogram showing cardiac chamber collapse. Treatment depends on the cause but often involves pericardiocentesis or surgical drainage of fluid to relieve pressure on the heart.
Introduction to cardiac tamponade by Dr. Sayeedur Rahman Khan Rumi. Discussion of its significance in cardiology.
Cardiac tamponade defined; symptoms include elevated pressures, hypotension, and rapid diagnosis needed.
Various acute causes like myocardial infarction, aortic dissection, and post-surgery complications.
Chronic causes include collagen diseases and infections such as viral, bacterial, and tuberculous.
Tamponade's low occurrence rate (0.12%) in coronary interventions, but high in-hospital mortality (42%).
Discusses the underlying mechanisms and effects of cardiac tamponade on heart function.
Physical examination signs include raised JVP, low BP, tachycardia, soft heart sounds, and potential rub.
Describes pulsus paradoxus, its normal variations, and its exaggerated response in tamponade.
Diagnostic methods including ECG findings, echocardiogram indicators, and Doppler studies.Management options range from observation, pericardiocentesis, to surgical interventions for fluid drainage.
Introduction
• Cardiac tamponadeis a hemodynamic condition
characterized by equal elevation of atrial and
pericardial pressures, an exaggerated inspiratory
decrease in arterial systolic pressure (pulsus
paradoxus), and arterial hypotension.
• If there is rapid accumulation, 200 ml fluid can
cause cardiac tamponande. However, if slow
accumulation of fluid occurs, 2000 ml may be
required for cardiac tamponade.
• This is an acute situation that requires quick
diagnosis and pericardial aspiration.
3.
Acute Causes
• MIwith rupture of ventricular wall
• Aortic dissection into the pericardial space
• After cardiac surgery
• Chest trauma
• After trans-septal puncture at cardiac catheter
• Uraemic patients undergoing haemodialysis (and
heparinization)
• Malignant disease and/or radiotherapy
• Patients on anticoagulants
• Associated with acute pericarditis
• Perforation of a coronary artery during PCI
• Cardiac tamponadeis an uncommon but
potentially lethal complication of percutaneous
coronary intervention.
• In one review of >25,000 interventions at a single
center over a 7-year period, the incidence of
tamponade was only 0.12%, but the in-hospital
mortality rate was 42%.
• The use of atheroablative therapy was associated
with a higher incidence of tamponade than
angioplasty and stenting alone.
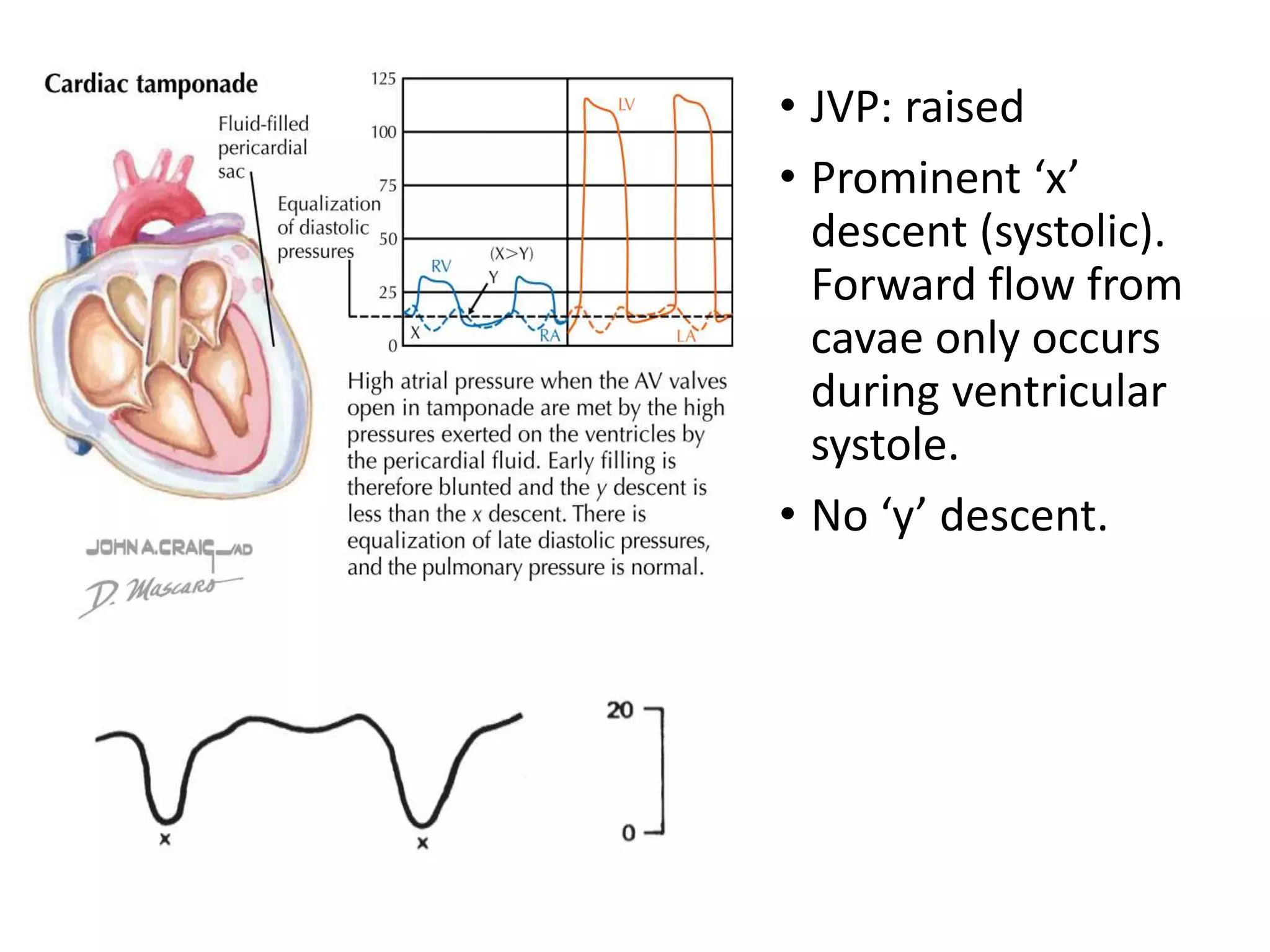
• JVP: raised
•Prominent ‘x’
descent (systolic).
Forward flow from
cavae only occurs
during ventricular
systole.
• No ‘y’ descent.
13.
• BP: low.May be
undetectable on
inspiration.
• Pulse: Sinus
tachycardia, low volume.
Pulsus paradoxus.
Heart sounds are soft.
There may be a
pericardial rub in
tamponade.
Oliguria or anuria rapidly
develops with
tamponade, and a brisk
diuresis occurs when
tamponade is relieved
14.
Pulsus Paradoxus
• Inhealthy individuals, systolic blood pressure may decline
by as much as 10 mm Hg during quiet inspiration.
• Pulsus paradoxus is an exaggeration of this normal
physiologic response.
15.
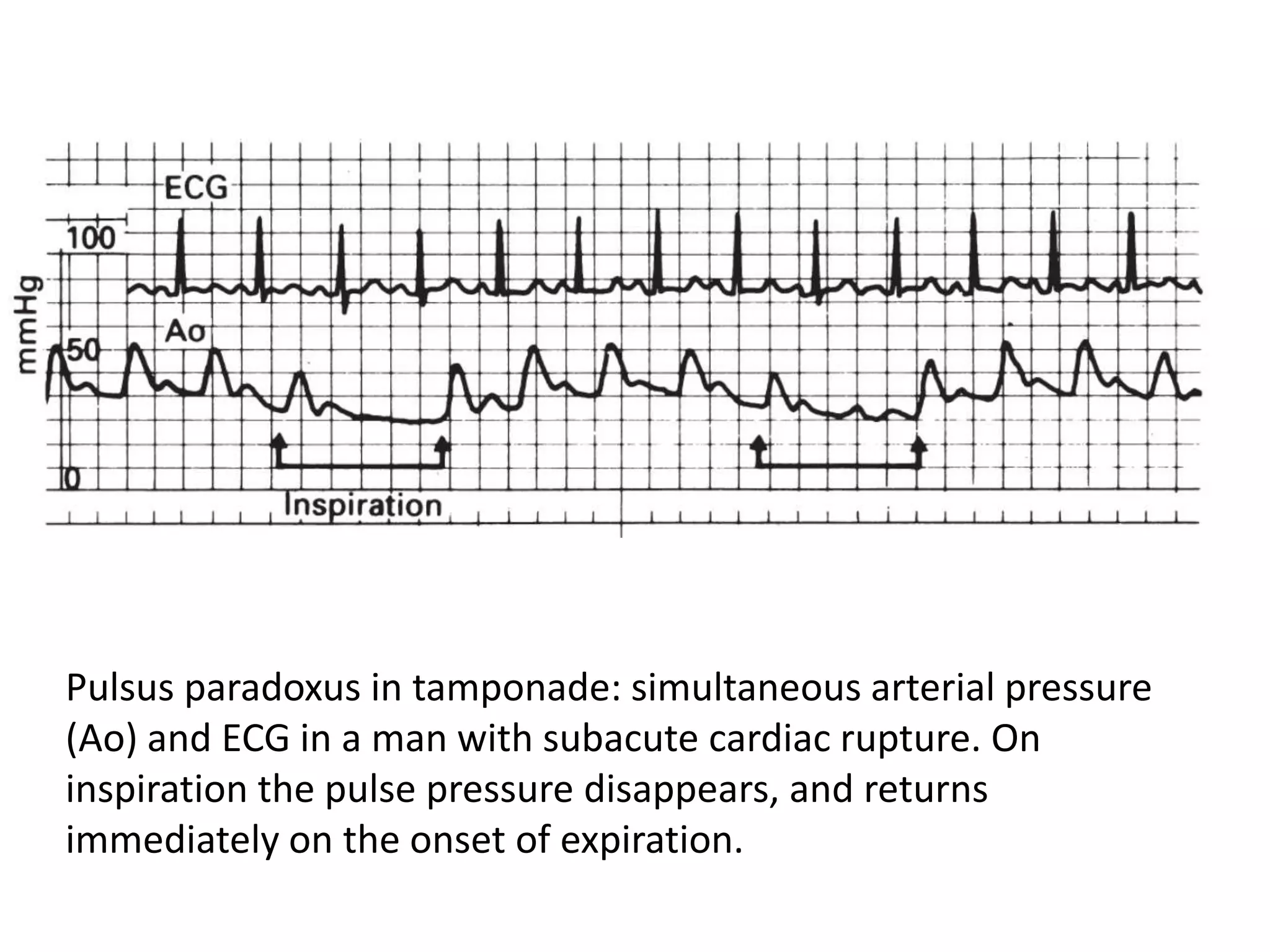
Pulsus paradoxus intamponade: simultaneous arterial pressure
(Ao) and ECG in a man with subacute cardiac rupture. On
inspiration the pulse pressure disappears, and returns
immediately on the onset of expiration.
Echocardiogram
• During inspiration,a greater than-normal increase in RV
dimension and decrease in LV dimension occur in many cases
of tamponade.
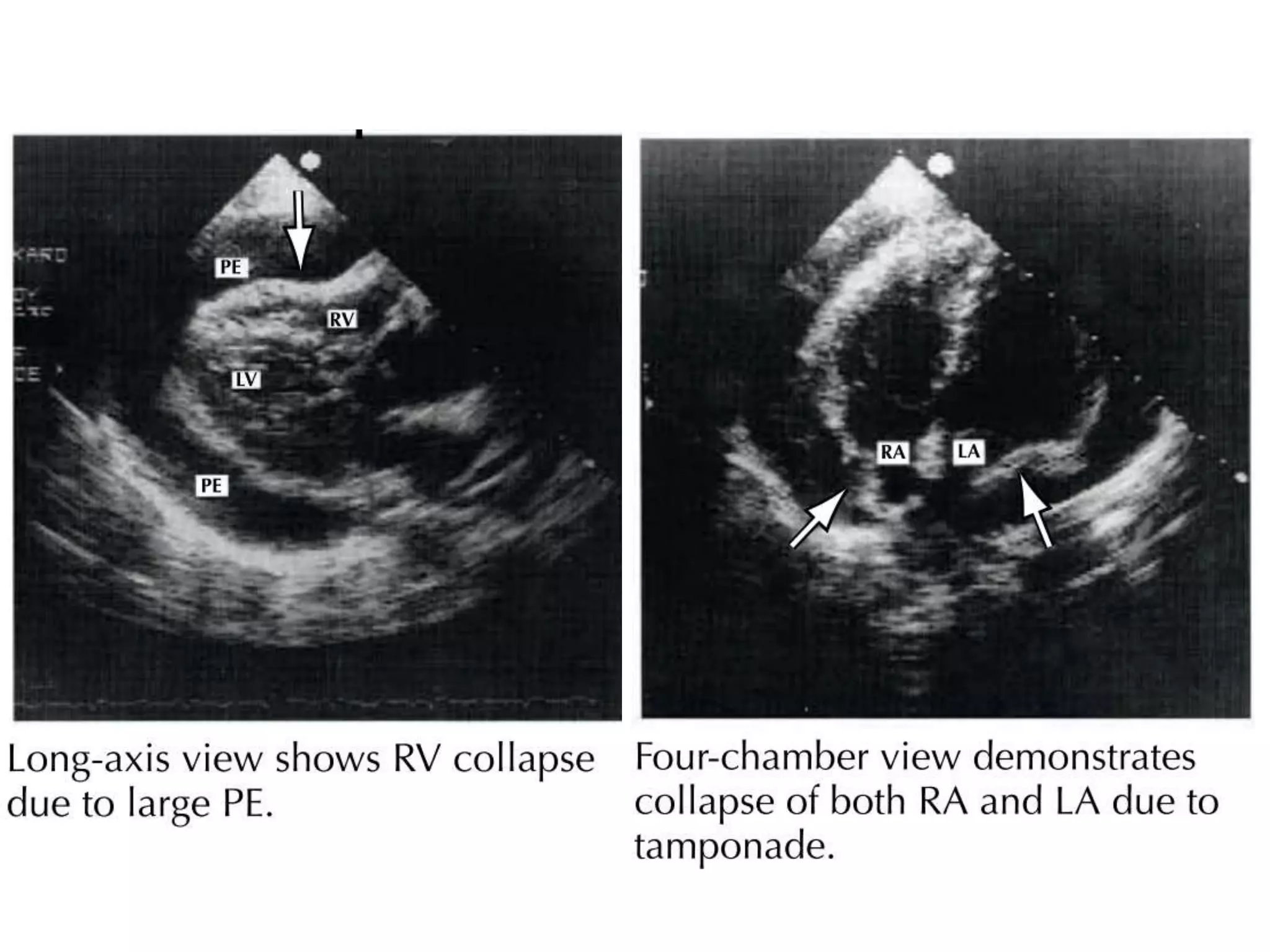
• RV diastolic collapse is sensitive to alterations in ventricular
loading conditions and may not be seen in the presence of
RV hypertrophy.
• In addition, collapse of the right heart chamber occurs with
smaller collections of fluid and higher pericardial pressures
when there is coexisting LV dysfunction. Late diastolic right
atrial collapse is virtually 100% sensitive for tamponade but
is less specific.
• Duration of right atrial collapse exceeding one-third of the
cardiac cycle increases specificity without sacrificing
sensitivity.
20.
Doppler echocardiogram ina patient with cardiac tamponade
showing inspiratory increase of tricuspid flow velocities
21.
Doppler echocardiogram ina patient with cardiac tamponade
showing expiratory increase of mitral and aortic flow velocities.
General management
• Themanagement of cardiac tamponade depends
upon clinical circumstances.
• In many cases,haemodynamic compromise may be
relatively mild and no action may be required other
than simple observation.
• Diuretics & vasodilator should be avoided.
• Further elevation of right sided pressures with
intravenous fluids may be of value and gain a
temporary improvement in cardiac output l
24.
Pericardiocentesis
• Needle pericardiocentesisis
often the best option when
the etiology is known and/or
the diagnoses of tamponade
is in question
• Pericardiocentesis is ill-
advised when there is <1 cm
of effusion, loculation, or
evidence of fibrin and
adhesion.
26.
Surgical drainage
• Althoughpericardiocentesis may provide effective
relief, percutaneous balloon pericardiotomy,
subxiphoid pericardiotomy, or the surgical creation
of a pleuropericardial or peritoneal-pericardial
window may be required.
• Surgical drainage is optimal when the presence of
tamponade is certain but the etiology is unclear.
• Open surgical drainage offers several advantages,
including complete drainage, access to pericardial
tissue for histopathologic and microbiologic
diagnoses, the ability to drain loculated effusions,
and the absence of traumatic injury resulting from
blind placement of a needle into the pericardial
sac.
27.
• Recurrent effusionsmay be treated by
• repeat pericardiocentesis,
• surgical creation of a pericardial window, or
• pericardiectomy.
28.
• Irrespective ofthe method of retrieval, pericardial
fluid should be sent for
• Hematocrit and cell count,
• Glucose,
• Gram stain,
• Ziehl-Neelsen stain,
• Cultures, and
• Cytology.
• Depending on the clinical circumstances, cytology,
tumor markers and carbohydrate antigens (for
suspected malignant disease), and adenosine
deaminase, interferon-γ, pericardial lysozyme, and
PCR analysis (for suspected tuberculosis) should be
obtained.