
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Cardiac tamponade
Similar to Cardiac tamponade (20)
Recently uploaded
Recently uploaded (20)
Cardiac tamponade
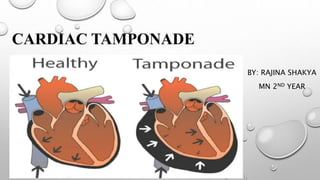
- 1. CARDIAC TAMPONADE BY: RAJINA SHAKYA MN 2ND YEAR
- 2. ANATOMY OF PERICARDIUM • Fibro-elastic sac that envelope heart • Two layers: • Outer: parietal pericardium (consists of fibrous and serous tissue ) • Inner : visceral pericardium (consists only serous tissue) also known as epicardium) • Space between two layers: pericardial space
- 3. CARDIAC TAMPONADE Cardiac: heart , tamponade: pressure Cardiac Emergency Cardiac tamponade is a life threatening condition where there is excess fluid accumulation in pericardial space which exerts pressure in the heart muscles. Or Compression of all cardiac chambers due to excessive accumulation of pericardial fluid leading to compromised cardiac output.
- 4. EPIDEMIOLOGY • Incidence : 2-5 cases per 10000 • 2% penetrating injuries result into cardiac tamponade • In children more common in boys, boys: girls 7:3 • In adults male: female = 1.25:1 • Cardiac tamponade related to trauma or HIV is common among young adults • US, 2018
- 5. ETIOLOGY • Cardiac tamponade develops due to pericardial effusion • Pericardial effusion: accumulation of excess fluid in pericardial space • Pericardial effusion may occur rapidly or insidiously • 19% of tuberculosis patients presented cardiac tamponade. (Shakya & Jha 2018)
- 6. ETIOLOGY Rapid pericardial effusion • Trauma : both stabbing and blunt • Post myocardial infarction • Heart surgery (open heart surgery, CABG) • Aortic dissection • Drugs and medications ( antihypertensives) Insidious pericardial effusion • Cancers ( lung or breast cancer) 30-60% • Infections (viral, bacterial, fungal) 5-10% • Uremic pericarditis (10-15%) • Hypothyroidism • Chronic inflammation of connective tissue (SLE, rheumatoid
- 7. PATHOPHYSIOLOGY Pleural effusion due to various causes exert pressure in heart walls Impairs relaxation and filling of the ventricles Chambers do not fill properly Less cardiac output (too little oxygen reaches the tissues) Hypotension increase heart rate ,faster breathing, feeling of panic, swollen neck veins
- 8. CLINICAL FEATURES • Pulsus paradoxus Beck’s triad • Distended jugular veins • Hypotension • Distant heart sounds Others • Tachycardia • Coughing , chest pain • Dyspnea(kussumaul’s breathing) • Weakness • Decreased urine output • Cyanosis of lips and nails • Confusion, dysphoria
- 10. DIAGNOSIS 1. History an d physical examination 2. Chest x-ray: cardiomegaly, bottle shape heart, chest wall trauma 3. ECG – tachycardia, low QRS complex voltage, electrical alternans, ST segment changes 4. Echocardiography: excess fluid, swinging heart 5. Cardiac catheterization (Swan-Ganz): pressure in all chambers are equal
- 12. LAB STUDIES • Creatine kinase and isoenzymes: elevated in MI and cardiac trauma • Renal profile : uremia if uremic pericarditis • Coagulation studies : helpful to determine bleeding risk to interventions • Antinuclear antibody assay and ESR: connective tissue disorder
- 13. TREATMENT • Immediate pericardiocentesis or pericardectomy and monitored in ICU • Supplemental oxygen • Volume expansion with blood plasma, isotonic normal saline to maintain adequate intravascular volume • Bed rest with leg elevation (increase venous return) • Intravenous Antibiotics • Management of underlying conditions
- 14. GUIDELINES OF EUROPEAN SOCIETY OF CARDIOLOGY, 2014 According to the guidelines, patients with suspected cardiac tamponade should undergo echocardiography without delay. After diagnosis, patients are scored according to disease etiology, clinical presentation, and imaging findings. A score of 6 or more requires the patient to undergo immediate pericardial drainage. A lower score indicates that drainage can be postponed for up to 12 to 48 hours.
- 15. PERICARDIOCENTESIS • Also known as pericardial tap • Is a surgical procedure( both diagnostic and therapeutic) in which abnormal or excessive fluid is removed from the pericardial sac. • Removal of 5- 10 ml may dramatic increase stroke volume and cardiac output by 25- 50%.
- 16. METHODS OF PERICARDIOCENTESIS 1. Emergency subxiphoid percutaneous drainage: blind technique, life-saving bed side procedure, subxiphoid approach is extra pleural, hence safest for performing without echocardiographic guidance. 4% mortality and 17 % complications 2. Echocardiography guided pericardiocentesis: done in cathlab, catheter is left for continuous drainage 3. Percutaneous balloon pericaridotomy: same as echo- guided, balloon is used for creating window for
- 18. INDICATIONS OF PERICARDIOCENTESIS • Pericarditis • Trauma • Surgery or other invasive procedures performed on the heart cancer and MI • Congestive heart failure • Renal failure
- 19. PRECAUTIONS • An echocardiogram should be performed to confirm the presence of the pericardial effusion and to guide pericardiocentesis needle during the procedure • Since there is risk of accidental puncture to major arteries or organs during procedure, surgical drainage may be preferred treatment option for pericardial effusion in non emergency situations
- 20. POST PERICARDIOCENTESIS CARE • Secure pericardiocentesis catheter in place • Periodically check for accumulation and drain • Repeat • Usually catheter is left in place for 1-2 days, within that period monitor serum cell counts, increased WBC indicates infection and requires immediate removal of catheter
- 21. SURGICAL MANAGEMENT • Surgical opening of a pericardial window: surgical opening of communication between pericardial space and intrapleural space • Open thoracotomy and pericardiotomy may be required in some cases • If recurrent cardiac tamponade or pleural effusion a. Sclerosing pericardium (instillation of stroids, tetracyclines or antineoplastic drugs in pericardial space via intrapericardial catheter
- 22. MEDICATIONS • Role of medications is limited • However by stimulating beta receptors , stroke volume and cardiac output can be increased • Dobutamine
- 23. COMPLICATIONS • Cardiac arrest • Myocardial infarction • Arrhythmias • Lacerations of heart muscles • Puncture or rupture of coronary arteries • Hemothorax, pneumothorax • Pneumo pericardium • Pulmonary edema , shock, death
- 24. NURSING MANAGEMENT • Assessment : • Assess the client status • Monitor hemodynamic status (pulse, heart rate, blood pressure, respiration rate) • Assess neurologic status (LOC, orientation, confusion, anxiety) • Cardiovascular assessment (heart rate, jugular vein distention, skin color)
- 25. NURSING DIAGNOSIS • Decreased cardiac output related to reduced ventricular filling secondary to increased intrapericardial pressure. • Activity Intolerance Related To Impaired Cardiac Performance
- 26. NURSING INTERVENTION • Monitor ECG for dysrhythmia (may occur due to MI), BP every 5- 15 min during acute phase, pulsus paradoxus via arterial tracing or during manual BP reading, urine output hourly. (Reduced renal perfusion) • Provide supplemental oxygen and IV fluids with two large bore IV lines • Provide pre and post op care ( assistance in investigations, imparting knowledge regarding disease, treatment and outcomes. • Medications like dobutamine to increase myocardial contractility
- 27. REFERENCES • Williams L. And Hopper P. Understanding medical surgical nursing. 4th edition. 2012. Jaypee brothers publications. India • SANDRA M. NETTINA. LIPPINCOTT MANUAL OF NURSING PRACTICE. 10TH EDITION(2014). WOLTERS KLUWERS HEALTH. INDIA • Brunner and Suddharth. Medical surgical nursing. • https://www.Slideshare.Net/anilkumargowda/cardiac- tamponade-79014744
Editor's Notes
- Pulsus paradoxus: abnormally large decrease in systolic blood pressure (>10 mmofHg) and pulse wave amplitude during inspiration and is a sign of cardiac tamponade that should be assessed every 4 hourly in a patient with pericarditis. At this pressure reading, if the cuff is not further deflated and a pulsus paradoxus is present, the first Korotkoff sound is not audible during inspiration. As the cuff is further deflated, the point at which the first Korotkoff sound is audible during both inspiration and expiration is recorded. Normally,decline during inhalation and increase during exhalation.
- Electrical alternans : different size of QRS complex
- Dobutamine ionotropic drugs