Download to read offline
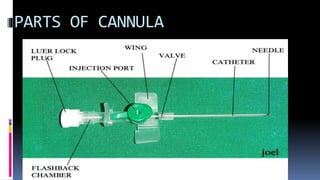
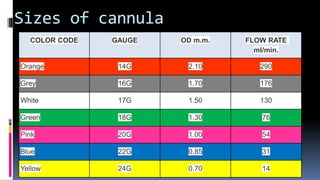
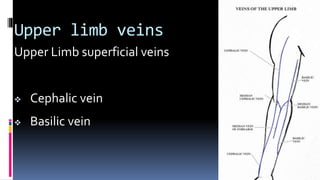
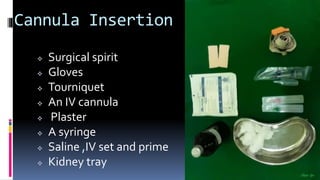








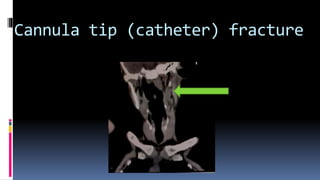
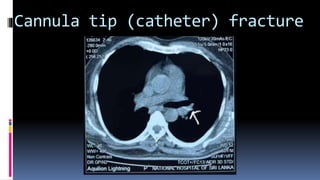



The document discusses cannulation techniques, the variety of intravenous cannulas, and their respective indications and complications. It highlights procedures for safe insertion, potential complications such as accidental intra-arterial cannulation and infection, and emphasizes prevention strategies. Key considerations include patient positioning, equipment readiness, and the importance of monitoring for adverse effects during and after cannulation.













































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








