This document describes the surgical procedure for repairing a symphysis pubis separation. The key steps involve:
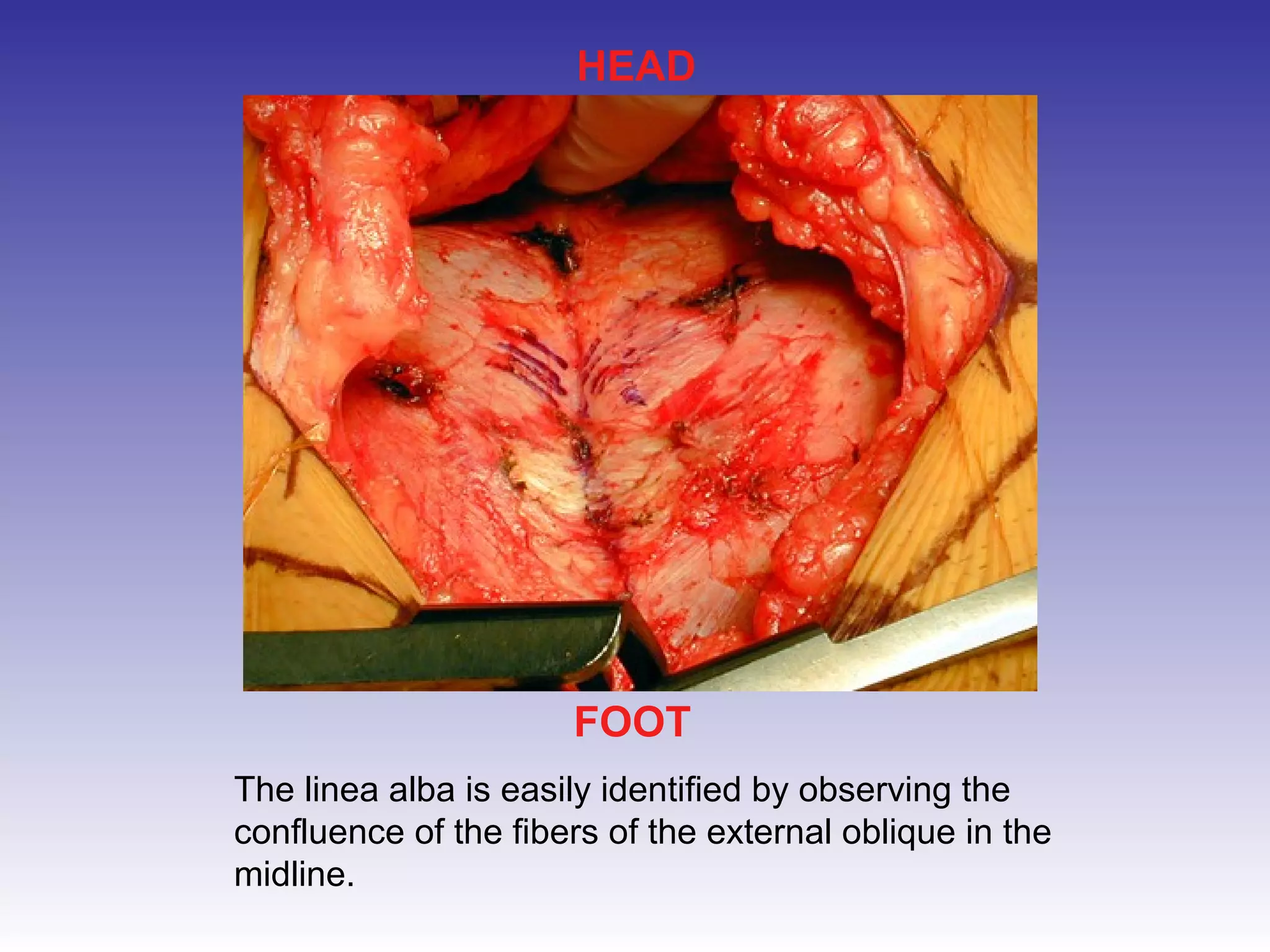
1) Making an incision above the pubic symphysis and retracting tissues to expose the injury;
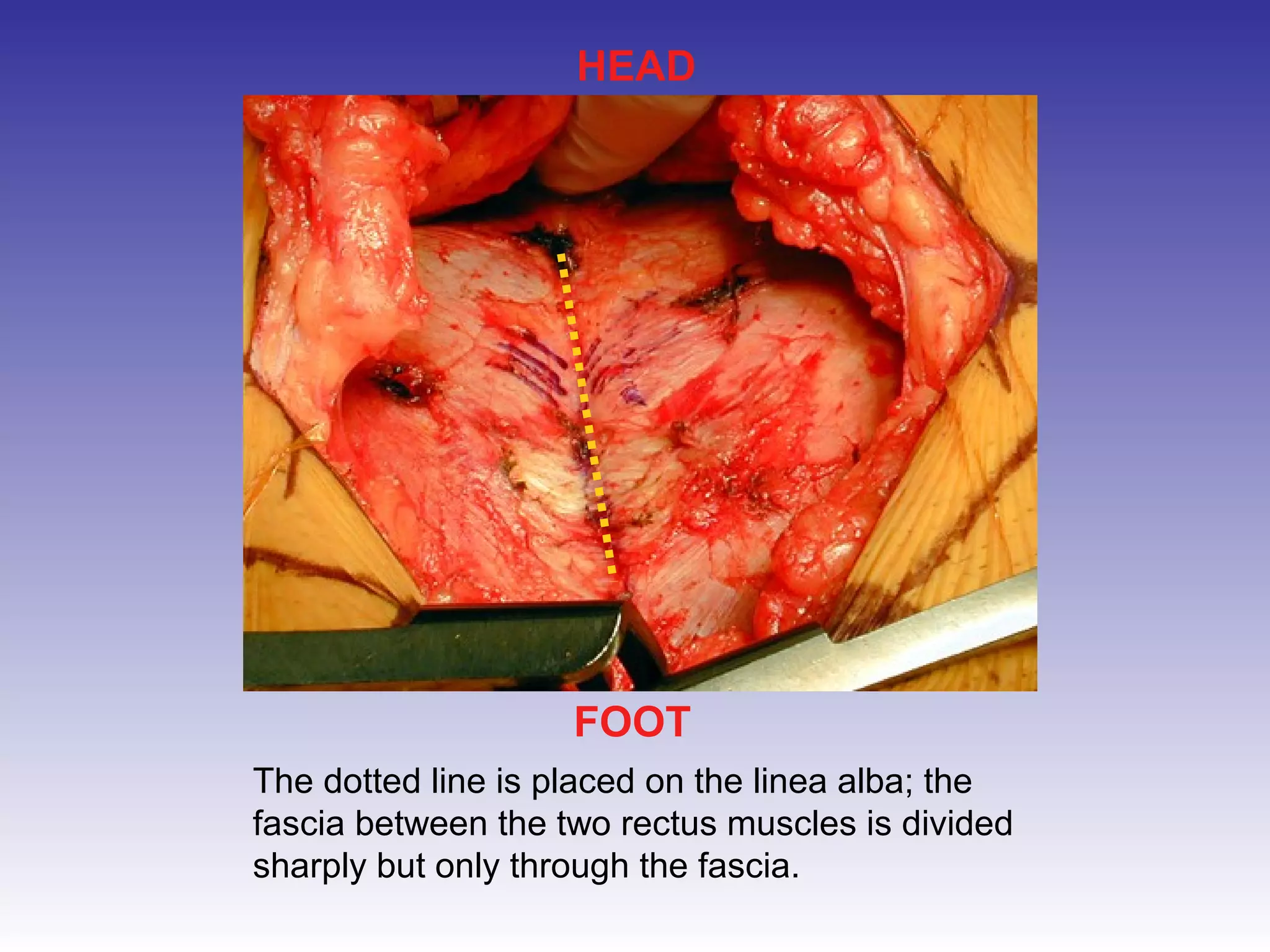
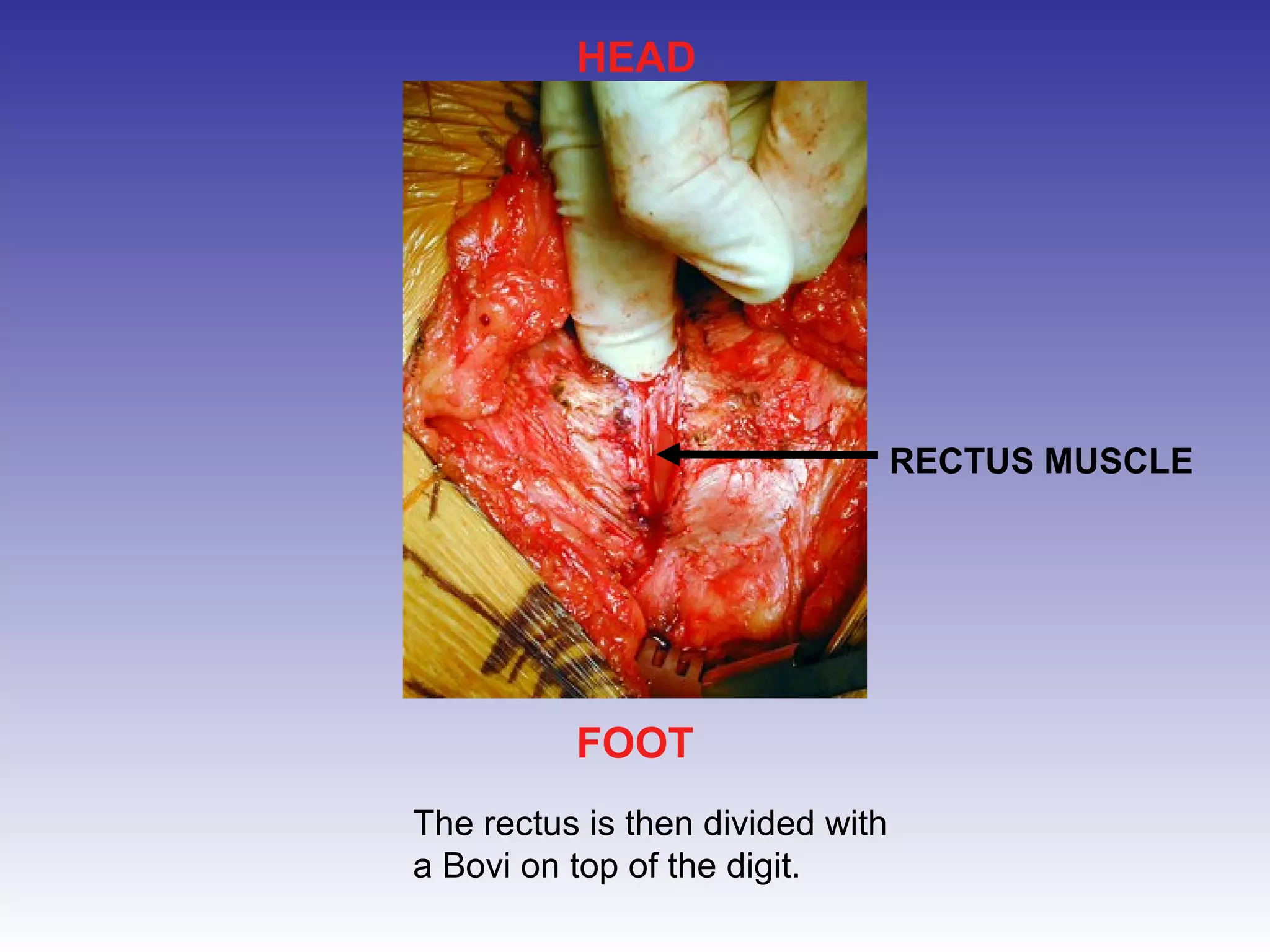
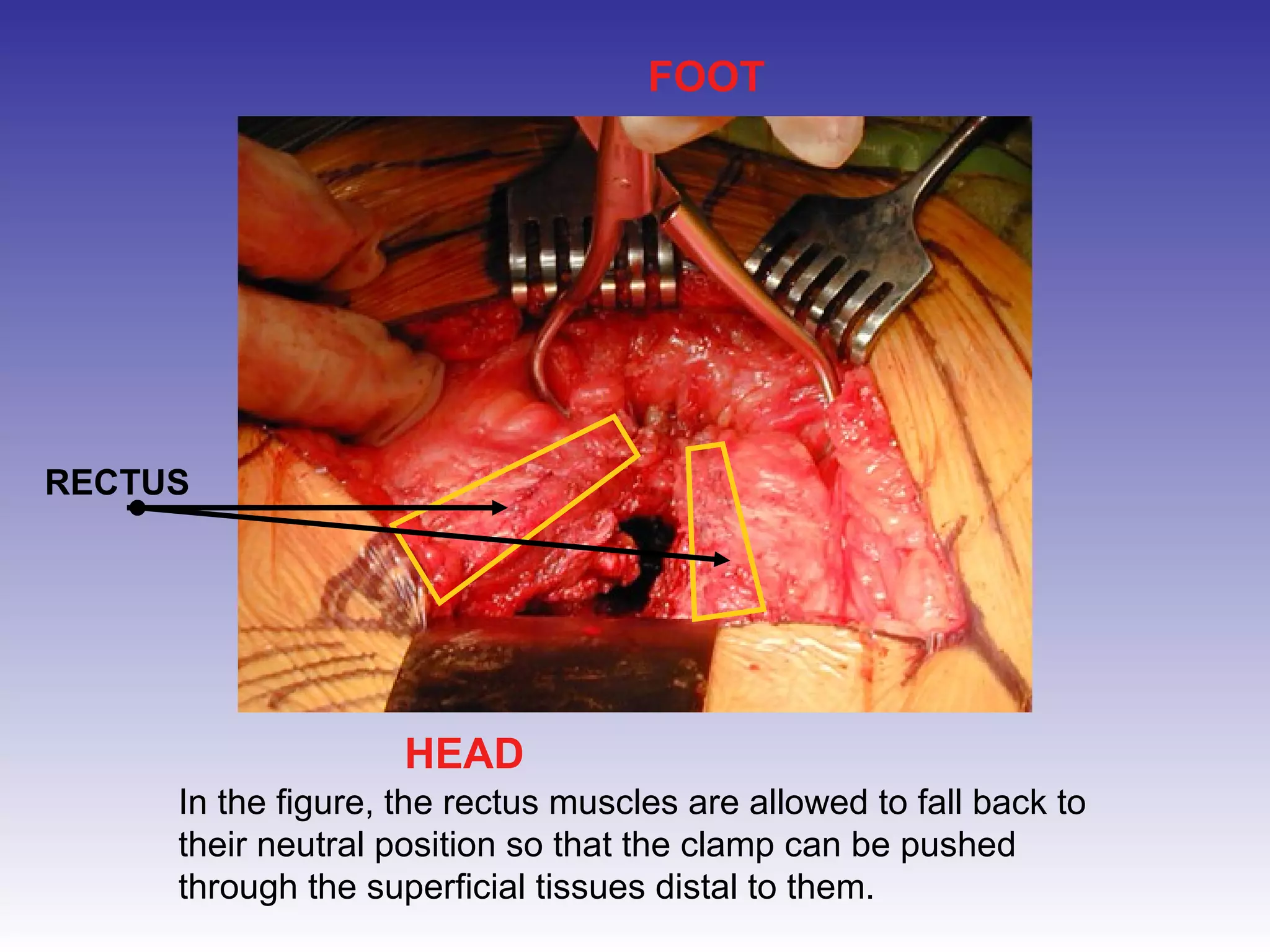
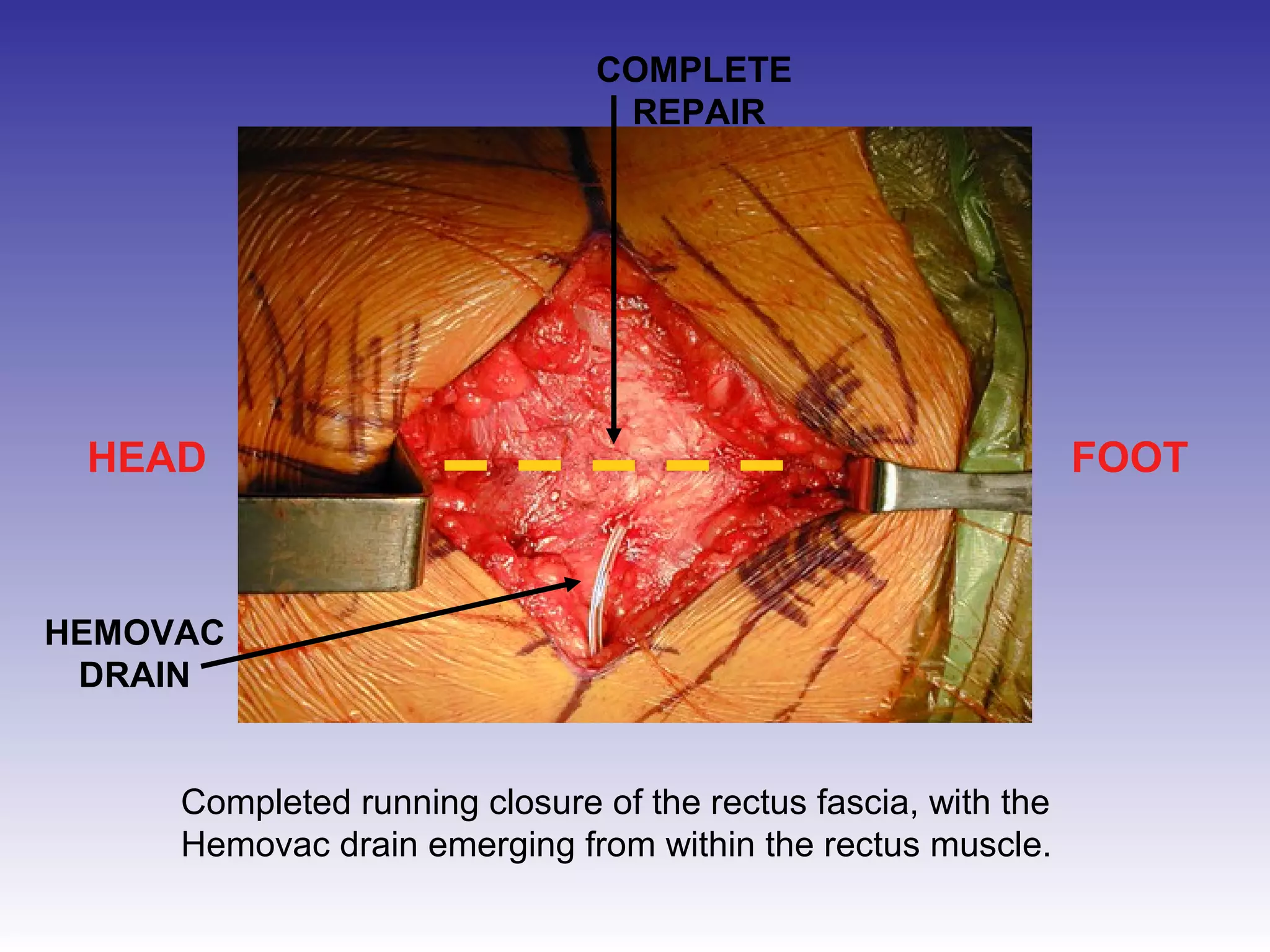
2) Splitting the rectus muscles and using retractors to further expose the pubic bones;
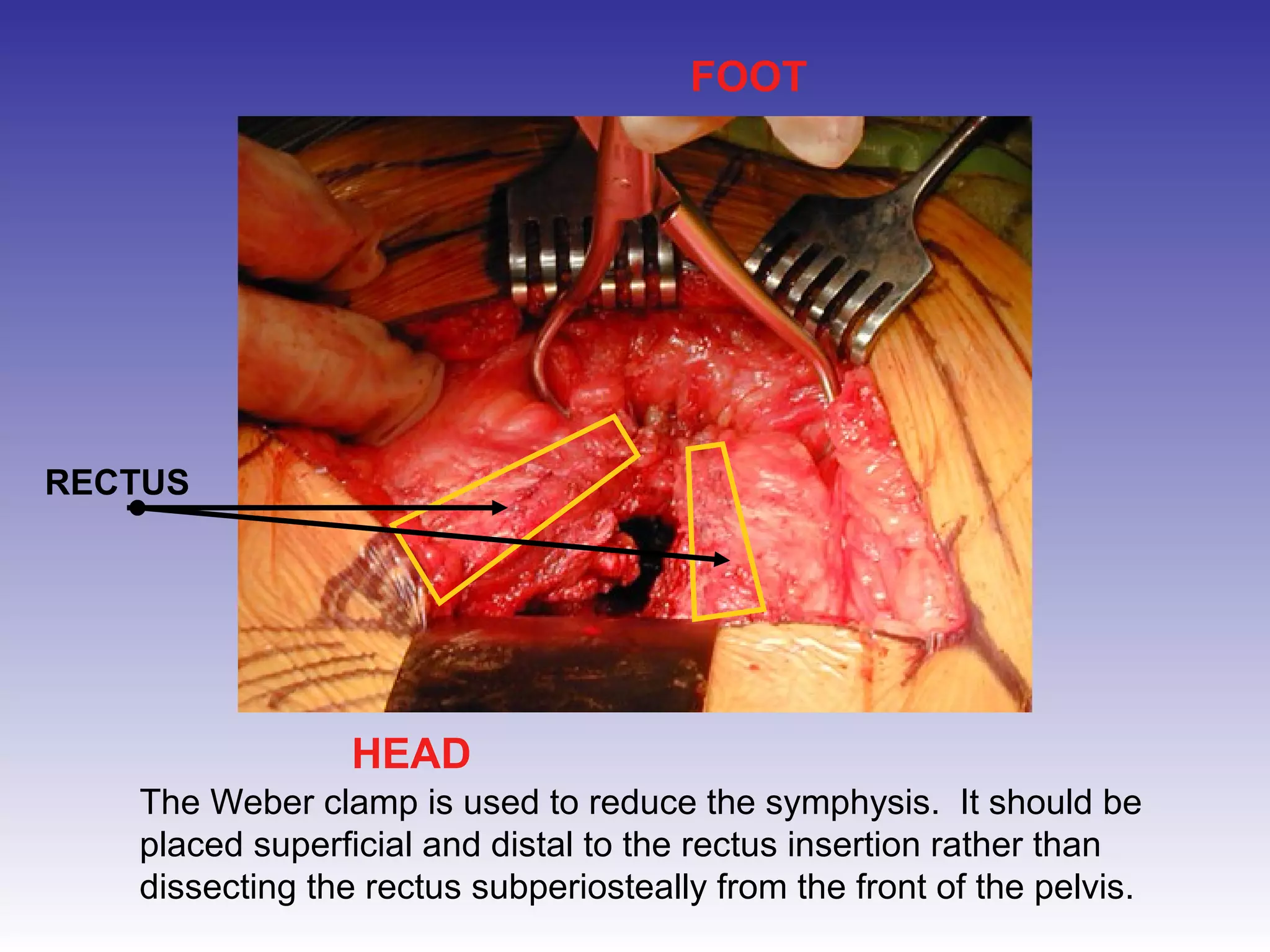
3) Reducing the separated pubic bones using a clamp;
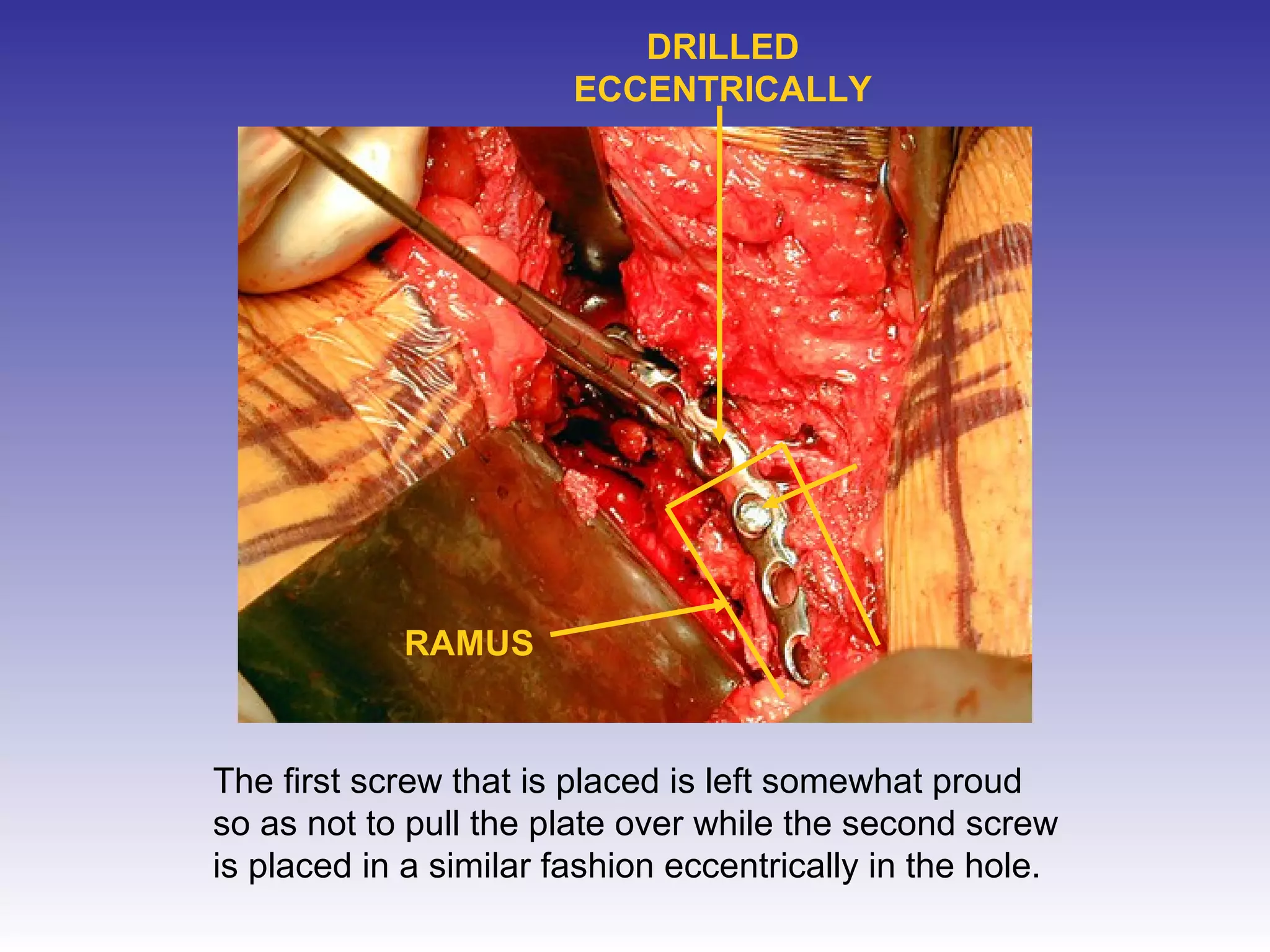
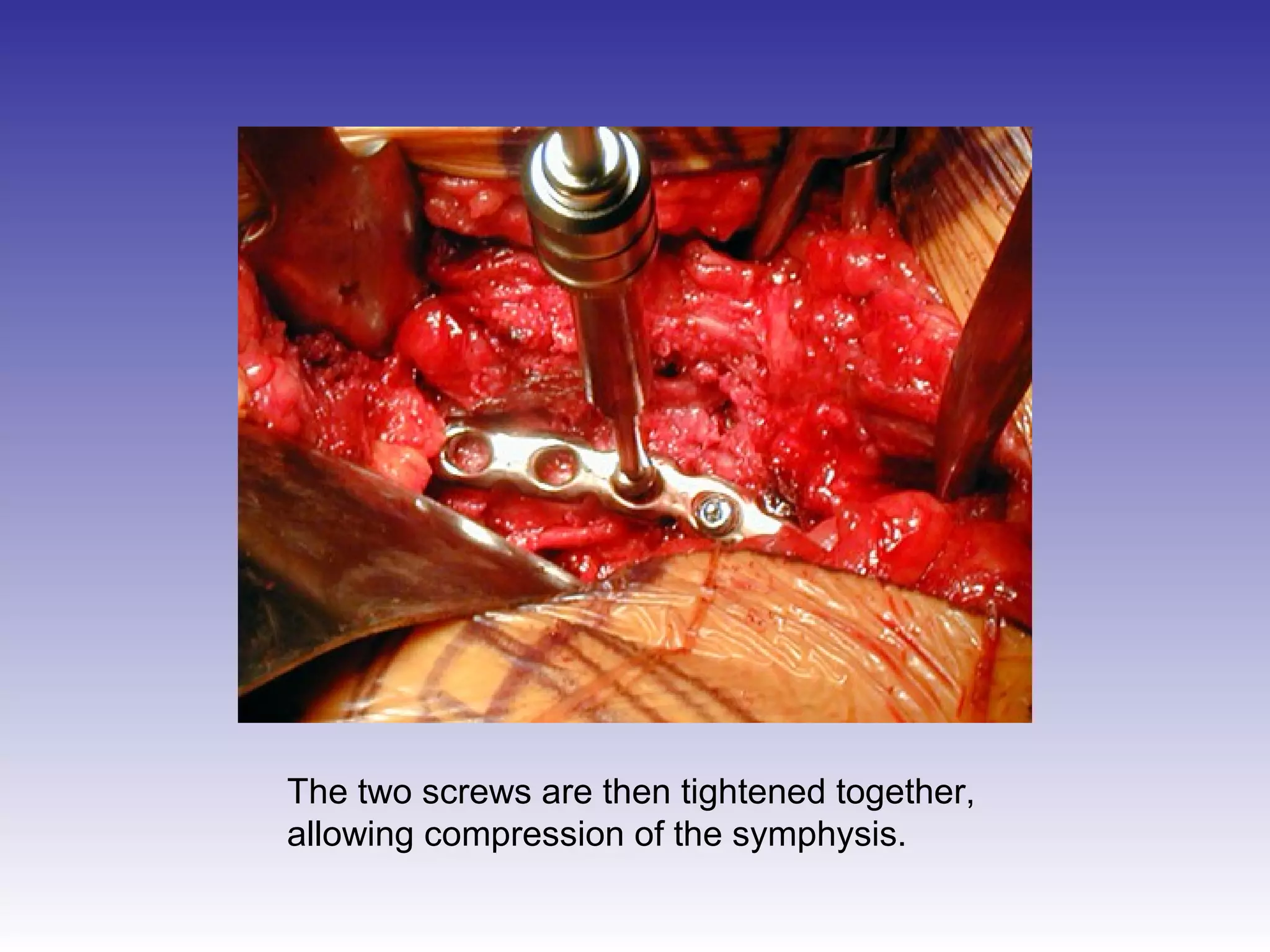
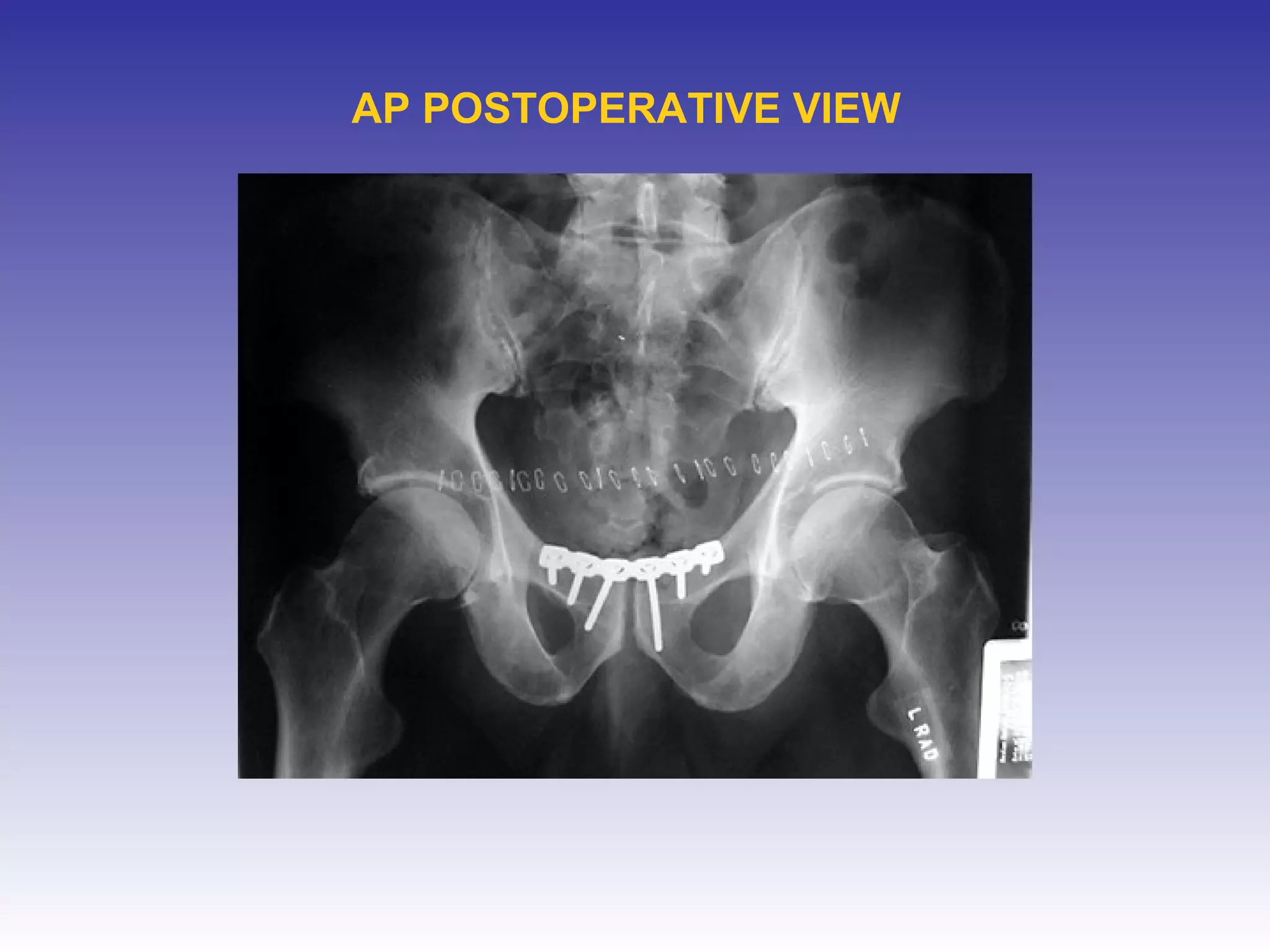
4) Placing a contoured metal plate and screws to stabilize the repaired symphysis.













































































































![Computer Networks 01[1 using all terms].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/computernetworks011-251214040533-327dd9f8-thumbnail.jpg?width=640&height=640&fit=bounds)






