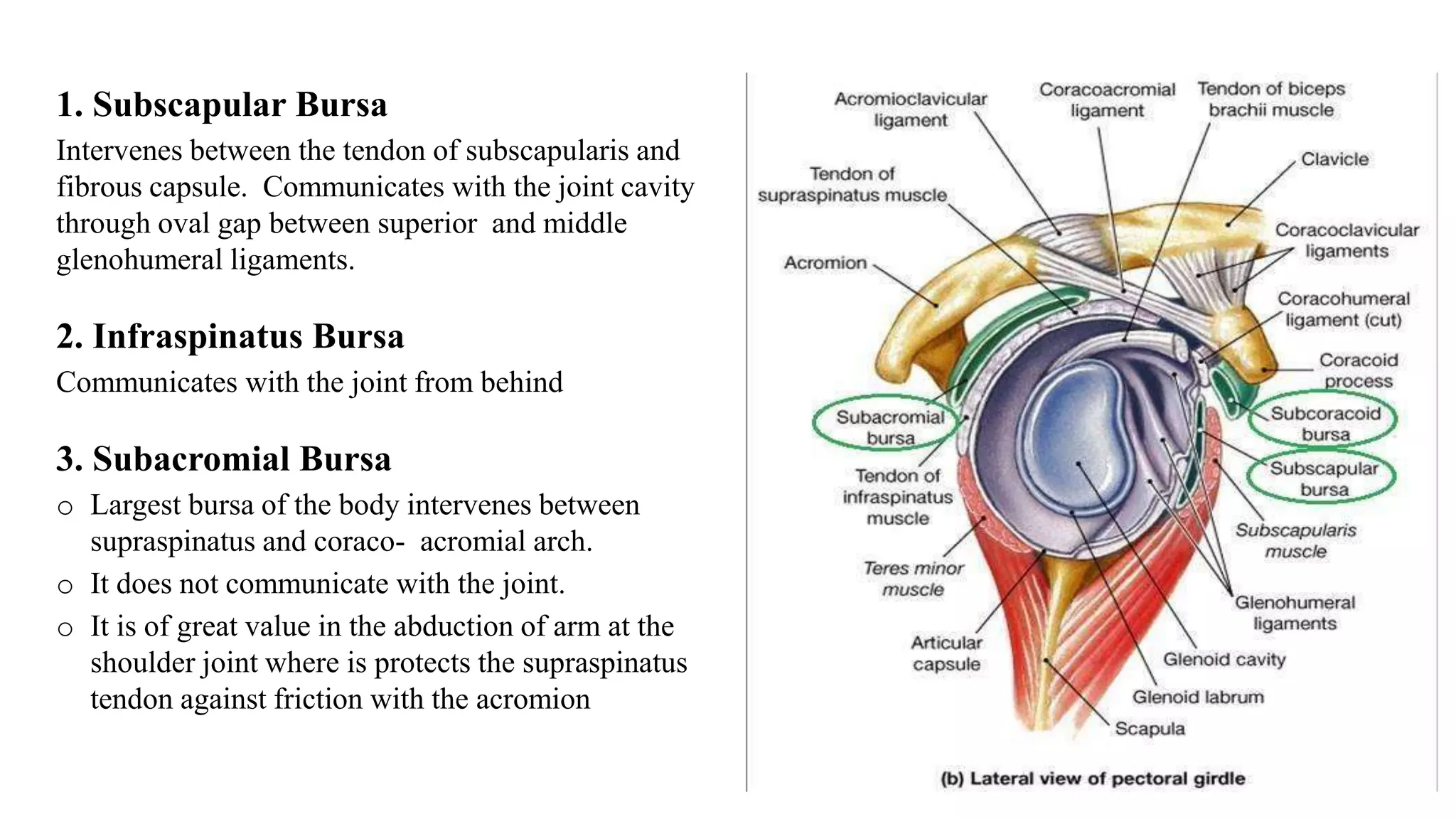
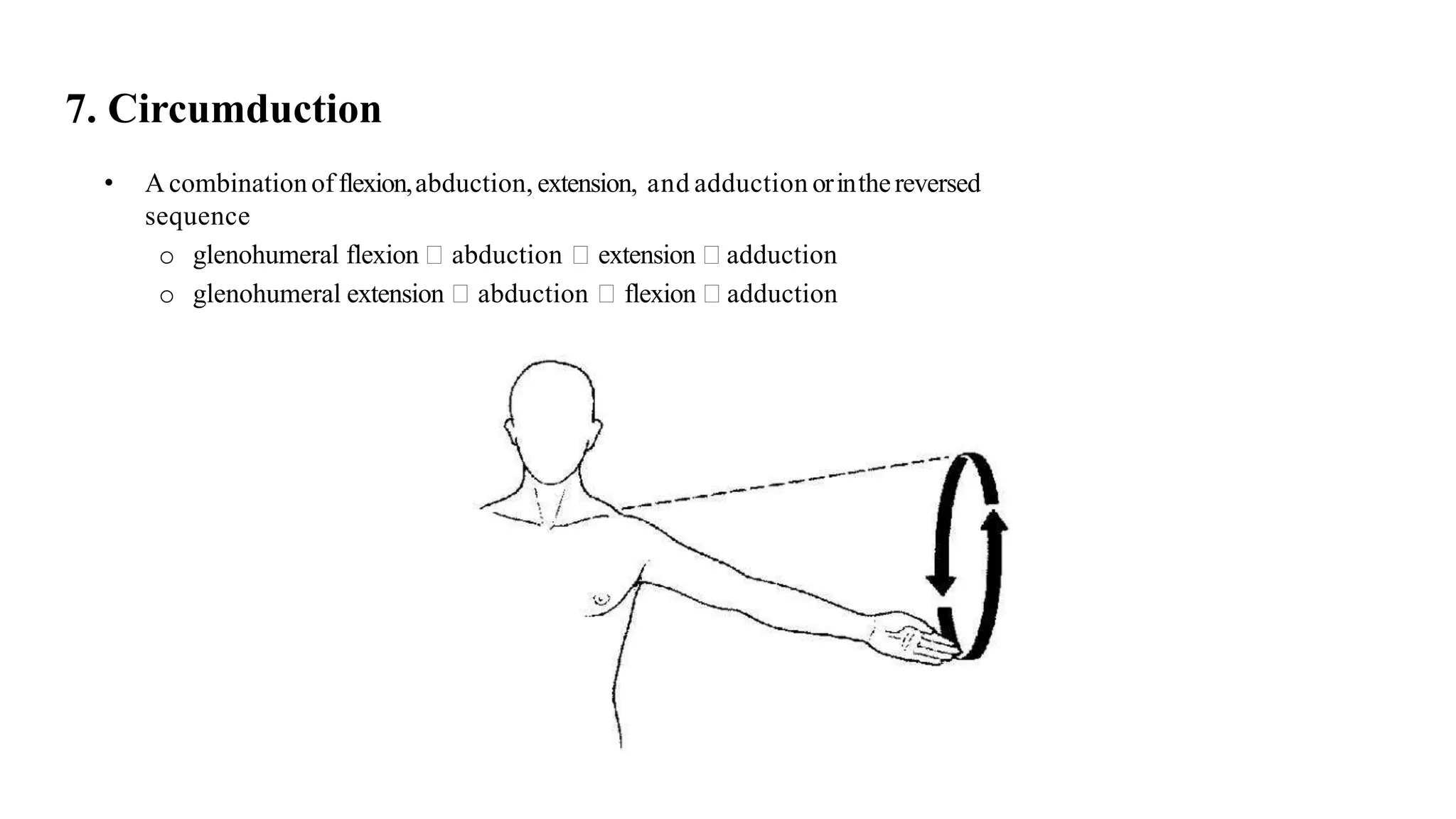
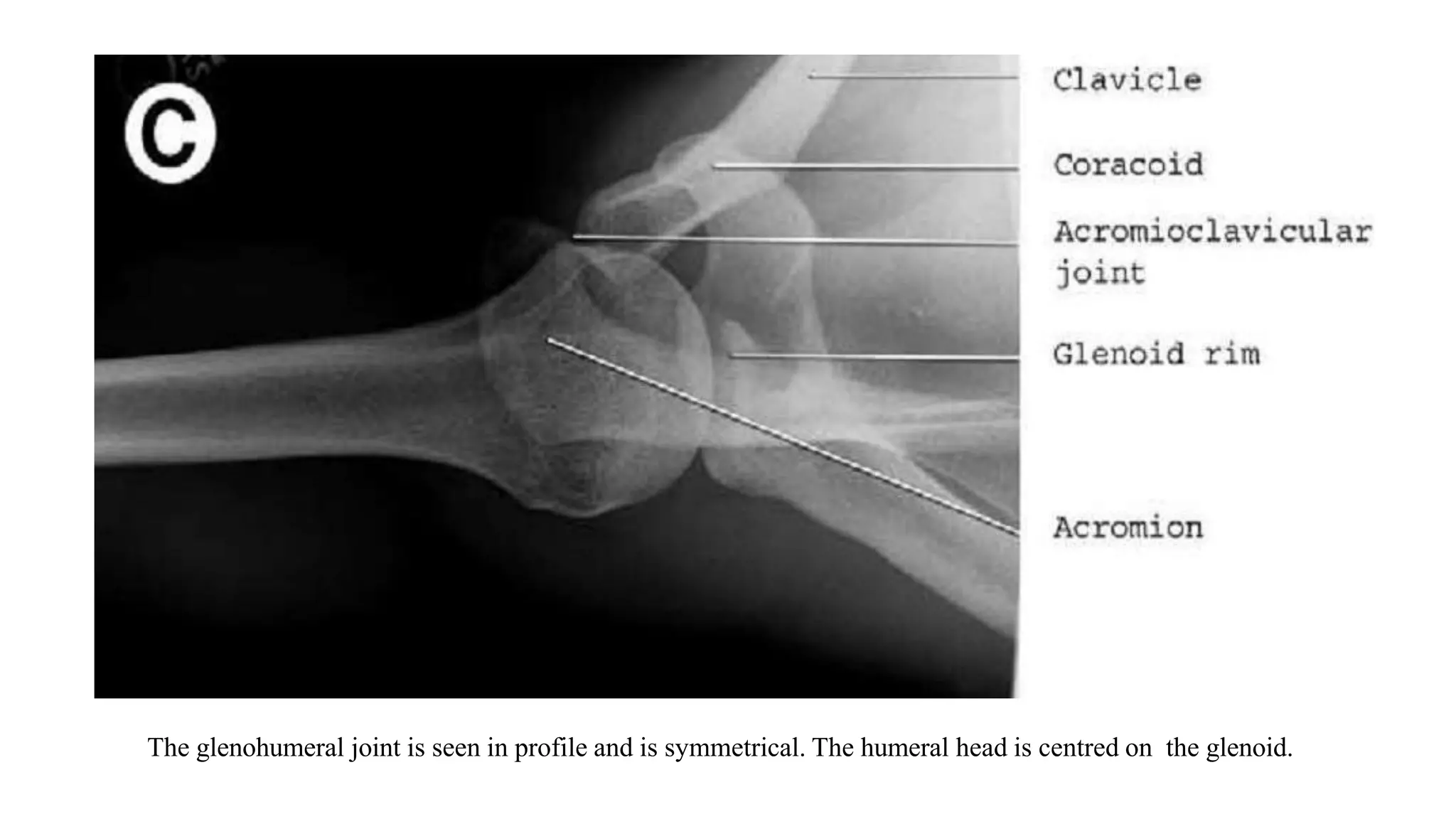
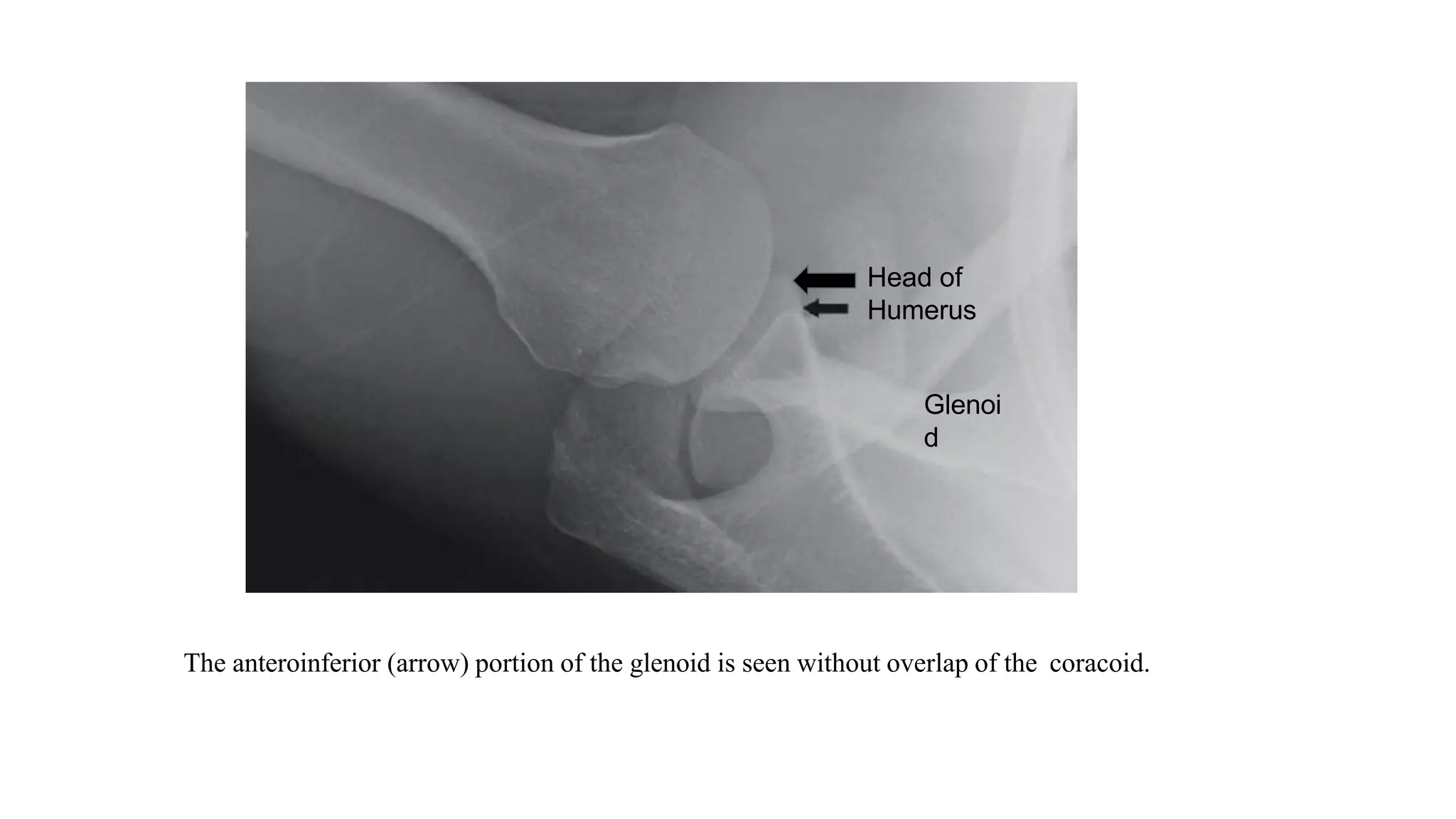
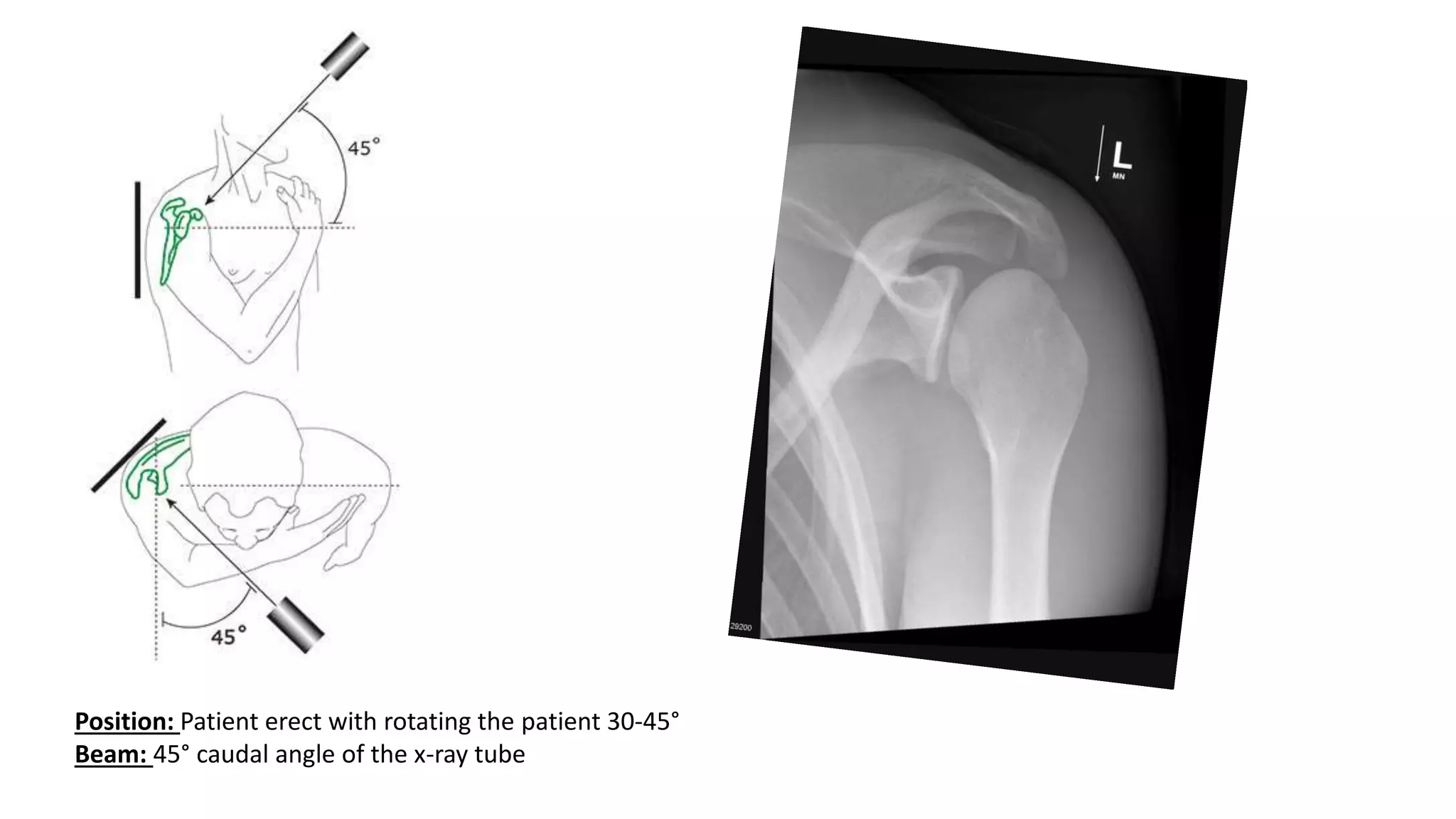
The document provides an in-depth overview of the anatomy and functioning of the shoulder joint complex, including details about its components (scapula, clavicle, and humerus) and associated ligaments and muscles that maintain stability and mobility. It describes four main joint types: glenohumeral, acromioclavicular, sternoclavicular, and scapulothoracic, alongside their specific movements, limitations, and supporting structures like the rotator cuff. Additionally, it touches on imaging techniques, especially radiographic methods, crucial for diagnosing various shoulder conditions.