Download as PDF, PPTX

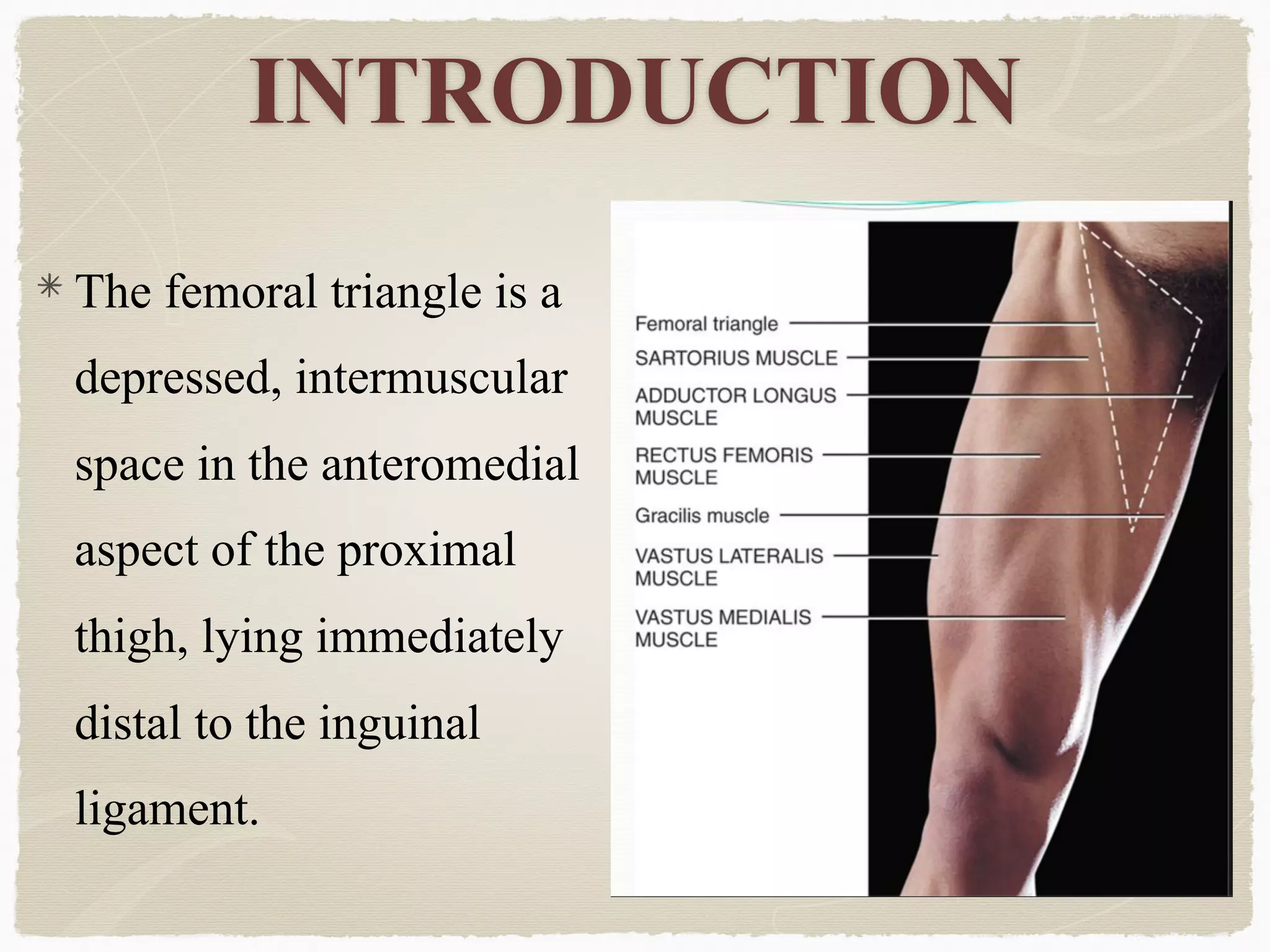













































The femoral triangle contains important structures in the upper thigh. It has boundaries of the inguinal ligament superiorly, the sartorius muscle laterally, and the adductor longus muscle medially. The floor contains muscles that aid in hip adduction. The femoral nerve provides sensation and motor function, and the femoral artery and vein are also located here, with the artery giving off deep branches. The structures of the femoral triangle are clinically relevant to conditions like varicose veins, hernias, and addressing muscle spasticity in cerebral palsy.









































































