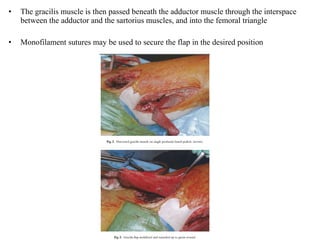
The document discusses several muscle flaps that can be used for coverage of infected vascular grafts, including the sartorius, gracilis, rectus femoris, tensor fascia lata, and rectus abdominis muscles. It also discusses using the greater omentum. Each option has advantages and disadvantages in terms of blood supply, size, and functional implications. The sartorius is frequently used due to its reliable segmental blood supply and proximity to the groin. The gracilis is suitable for smaller defects while the rectus femoris and tensor fascia lata are good for more extensive coverage.